

- Thread starter
- #561
Why thank you Shed. 
How To Use Progressive Web App aka PWA On 420 Magazine Forum
Note: This feature may not be available in some browsers.
Description | English: This is a diagram of a typical central nervous system synapse. The presynaptic and postsynaptic neuron are on top and bottom. Mitochondria are light green, receptors dark green, postsynaptic density is in grey, Brown pyramids represent protein clusters composing the active zone, cell adhesion molecules are brown rectangles, synaptic vesicles are tan spheres, endoplasmic reticulumis the tan structure on the bottom left. |
| Date | 5 April 2011 |
| Source | Own work |
| Author | Curtis Neveu |
 ) on the safety of combining St. John’ Work with Cannabis sativa.
) on the safety of combining St. John’ Work with Cannabis sativa. 
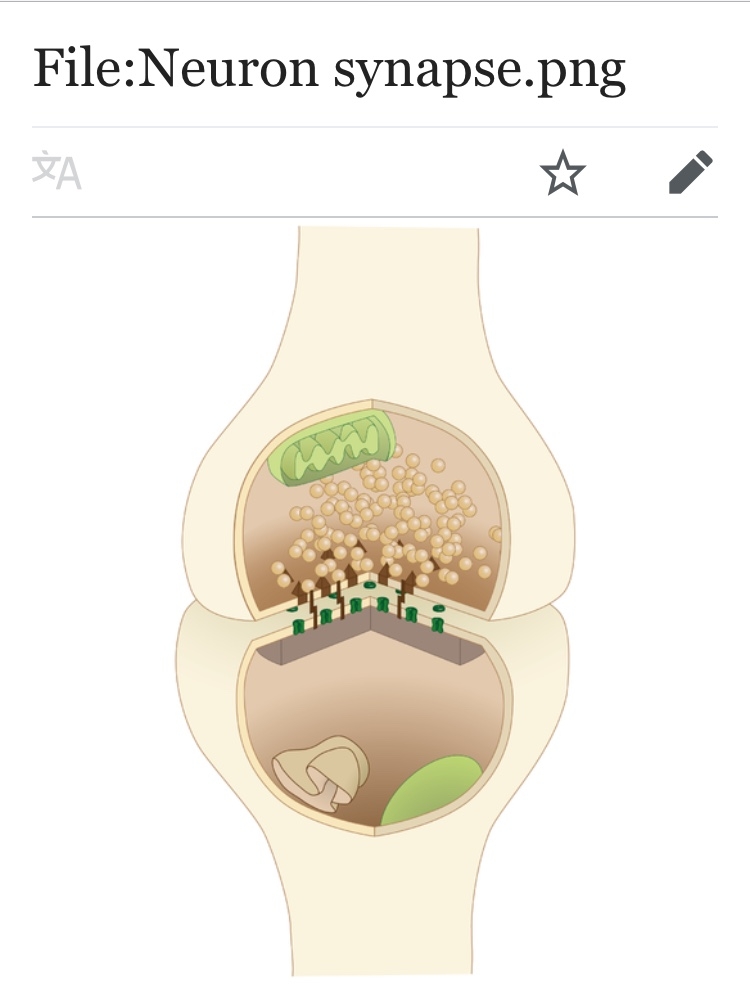
DescriptionEnglish: This is a diagram of a typical central nervous system synapse. The presynaptic and postsynaptic neuron are on top and bottom. Mitochondria are light green, receptors dark green, postsynaptic density is in grey, Brown pyramids represent protein clusters composing the active zone, cell adhesion molecules are brown rectangles, synaptic vesicles are tan spheres, endoplasmic reticulumis the tan structure on the bottom left. Date 5 April 2011 Source Own work Author Curtis Neveu
 Nerve cells also have tiny electrical charges and it passes from positive to neg, as it transfers signals from cell to cell. so, biochemical electrical activity occurs in our bodies ,just as an electric motor uses a battery or grid current, our body derives what it needs from cellular processes that utilize bio chemical electric power from what we and our environment feeds it.
Nerve cells also have tiny electrical charges and it passes from positive to neg, as it transfers signals from cell to cell. so, biochemical electrical activity occurs in our bodies ,just as an electric motor uses a battery or grid current, our body derives what it needs from cellular processes that utilize bio chemical electric power from what we and our environment feeds it.  sometimes I feel like a walking battery that needs charging or sometimes all charged up. Too often my battery terminals are clogged up with man made crap and I need some maintenance. Cannabis to the rescue! Helps me almost every time!
sometimes I feel like a walking battery that needs charging or sometimes all charged up. Too often my battery terminals are clogged up with man made crap and I need some maintenance. Cannabis to the rescue! Helps me almost every time! CBD is great,but it works better with THC at it's side! Walnut cco brownies and ice cream is great for recharging my batteries!
CBD is great,but it works better with THC at it's side! Walnut cco brownies and ice cream is great for recharging my batteries!This is not the first study to herald the medicinal qualities of marijuana. Medical News Today reported last month that chemicals within the plant may protect the body against multiple sclerosis."MicroRNA therapeutics is an important, rapidly growing area with major pharmaceutical companies getting into this discovery and development. While our study identifies the molecular mechanism of immune-altering effects of marijuana, select microRNA identified here could serve as important molecular targets to manipulate MDSC activity in cancer and inflammatory diseases."
They had tried her on methotrexate and it didn’t agree with her, some flares took as high as 80 mg of prednisone to for around a year I believe to get it under control then took a while to slowly taper her down to where she is now at 10mg a day and keeps the flares at bay but she can still feel the pressure in her eye. Humira is also given, this is crazy to read another case with pretty much exact same symptoms... she’s been dealing with this for over 2 years now unfortunatelyI stumbled upon this case study and thought it might be interesting to see how a case is handled conventionally.
Source
A Painless Scleritis?
Faye Therese Gamboa, O.D.
Resident Optometrist - Captain James A. Lovell FHCC (708) 620-9295 // fgamboa23@yahoo.com
ABSTRACT: This case presents an atypical scleritis with hyperemia, decreased vision, and no pain, presumed to be secondary to immune-compromise. Proper dose of non-steroidal anti- inflammatory drugs or oral steroids is imperative to protect vision.
I. Case History
a. 68 year-old Caucasian Male
b. Painless, progressive red eye with mild irritation and associated watering OD. Started 3 mo ago. Separately, the patient notes mild crusting AM with foreign body sensation OD as well. No fevers, night sweats, weight loss, diplopia, light sensitivity, itching, burning, discharge, change in vision as. Denies previous red eye episodes OU.
c. Last eye exam:
1 month ago with optometrist who prescribed antibiotic drops that did not help d. Pertinent Medical History:
Ulcerative Colitis (UC) x 13-14 yrs. – in remission
Anemia
e. Systemic Medications:
Humira® immunosuppressive injections sig 2 wks x 1 yr. for UC OTC supplements:
Multivitamin
Folic Acid 1mg
Cyanocobalamin
B12
Fish Oil 1000 mg
Flaxseed
Glucosamine
f. Family History:
Thyroid disorder – daughter
g. Social History
Quit smoking ~ 45 yrs. ago
Social drinker
Infrequent marijuana use
h. Retired Engineer x 30 yrs.
II. Pertinent Findings
a. Clinical (Initial Visit)
1. Entering VA (sc) 20/20 OD, 20/20 OS2. Pupils, EOM’s, Confrontation VF’s: WNL OD, OS3. Slit lamp:OD: 2-3+ diffuse conjunctival injection, tr-1+ diffuse papillae on upper/lower lid, no corneal involvement, (-) cell/flare, (-) foreign body OS: normal findings
4. Goldmann IOP: 11mm Hg OD, 11 mmHg OS
5. Blood pressure: 134/83 mmHg
6. External exam:OD: mild injection along lid margins, no exophthalmos, mild tenderness over ethmoid sinus only (-)frontal sinus, no preauricular lymphadenopathy OS: within normal
7. DFE: within normal (-)vitritis/retinopathy OU
b. Follow-up (2 weeks later) – after patient prescribed FML QID OD
1. All findings stable except:A. Entering VA (sc): 20/25 OD, 20/20 OS B. Slit lamp:OD: 1-2+ edema/erythema sup./inf. lid, (-) tenderness, 3+ deep, diffuse conjunctival injection, no corneal involvementOS: within normal
c. Follow-up (1 mo later) after prescribed Naproxen po QID
1. All findings stable except:A. Entering VA (sc): 20/30 OD, 20/25 OS B. Slit lamp:OD: 1-2+ edema/erythema superior and inferior lid, (-) tenderness, 2+ deep conjunctival injection temporal and nasal, 1+ conjunctival injection superior and inferior, no corneal involvementOS: within normald. Work-up
1. No Fluorescein staining on cornea OU at all visits2. Mild blanching with phenylephrine 2.5% but not completely OD at all visits 3. CRP within normal range one month prior to initial visit4. Vitamin D, 25 OH levels inadequate two months prior to initial visit
III. Differential Diagnosis
a. Scleritis
b. Episcleritis
c. Allergic Conjunctivitis
IV. Diagnosis and Discussion
a. Diagnosis
1. Diffuse Anterior Scleritis OD secondary to Ulcerative Colitis and probable immunosuppression
b. Ulcerative Colitis
1. Form of chronic inflammatory bowel disease (IBD)
A. HLA B-27+
2. Extra-intestinal manifestations are common. Ocular symptoms occur in 2-5% of patients with IBD. (7).A. EpiscleritisB. ScleritisC. Uveitis
c. Scleritis is an intense inflammation of the sclera that is often painful and can result in blindness.
1. Diagnosis is based upon clinical presentation: scleral inflammation with involvement of the superficial and deep episcleral venous plexuses. (5)
A. Phenylephrine 10% can be instilled to rule out episcleritis. (5)
2. Pain is almost always present, but can be absent if the patient is currently on immunosuppressive treatment. (5)
3. * Scleritis can be the first manifestation in 20% patients with systemic autoimmune disease. (5)
4. Types:A. Anterior or PosteriorB. Diffuse or NodularC. Necrotizing or Non-necrotizingD. * Diffuse anterior scleritis is the most common in about 45-61% of all cases. (5)
5. One case report presented a patient with very similar ocular symptoms as the case above and was also diagnosed with a painless posterior scleritis. (2)
d. Humira® (Adalimumab)
1. Tumor necrosis factor (TNF) inhibitors prevent TNF from inducing systemic inflammation caused by macrophages, CD4+ lymphocytes, and natural kills cells (1).A. Use of tumor necrosis factor inhibitors has been proven to decrease ocular inflammation, particularly Infliximab and Adalimumab. (1)B. Adalimumab is a humanized monoclonal antibody that recognizes and binds to TNF. (1)C. It is FDA approved for the treatment of ulcerative colitis. (1)D. It is given subcutaneously with a loading dose of 80mg, and then 40 mg every week or 20 mg every two weeks. Weekly dosing may be required for ocular disease. (1)E. Humanized to decrease the risk of developing antibodies to the TNF inhibitor and thus decreasing its efficacy. (1)F. No current studies that evaluate adalimumab as effective systemic treatment for scleritis and systemic effects limit their use. (1)Local administration is preferred, but may not be effective (4)1. One case report of significant improvement of a nodular scleritis in a patient diagnosed with rheumatoid arthritis (6)2. Difficult to proper assess effectiveness of systemic therapy due to small incidence, range of disease, and low pharmaceutical interest. (3)B. Topical corticosteroids are not as effective. 2. Oral SteroidsA. Prednisone 1mg/kg/day 3. ImmunosuppressantsA. MethotrexateB. AzathioprineC. Cyclophosphamide4. Biologic AgentsA. TNF inhibitors1. Infliximab2. Adalimumab
5. SurgeryA. Cataract removalB. Transplantation if perforation
6. Preventative Care and Maintenance through Diet (8)
A. "IBD-AID" diet - consists of lean meats, poultry, fish, omega-3 eggs, select sources of carbohydrate/fruits/vegetables, nut and legume flours, limited aged cheeses, fresh cultured product rich with probiotics, prebiotics that contain beta-glucans and inulin are suggested. (8)B. Vitamin D as protective measure. (9)1. Natural Vitamin D through sun exposure2. Cholecalciferol supplementation3. In this particular case, the patient was Vitamin D deficent on testing 1 month prior to reported symptoms.C. Fish Oil (10)
b. This patient was started on Naproxen 250mg po QID and Omeprazole 20mg po QD.
1. Mild resolution of scleritis after one month of follow-up. Still no pain.2. We believe that the patient is immunocompromised and, thus, delayed resolution of the patient’s ocular condition is expected.3. Current Vitamin D, 25 OH levels results still pending for this patient. We expect mildly higher levels due to increased sun exposure of summer. However, it is likely not adequate.4. Upon next follow-up, we expect continuous improvement of this patient's ocular condition and will determine proper diet and Vitamin D and Fish oil supplementation for long-term preventative care.
VI. Conclusion
a. Scleritis is a common extra-intestinal manifestation of Ulcerative Colitis. It is important to confirm the diagnosis and classification. Furthermore, it is important to determine complications and evaluate for an underlying cause, especially if there is a systemic etiology. (5)
b. Optometrists can play strong role in quickly diagnosing and treating this condition with prompt work up and proper referral to prevent severe vision loss.
c. In addition, as general physicians we can also consider determining natural and safe supplementation for preventative care.

They had tried her on methotrexate and it didn’t agree with her, some flares took as high as 80 mg of prednisone to for around a year I believe to get it under control then took a while to slowly taper her down to where she is now at 10mg a day and keeps the flares at bay but she can still feel the pressure in her eye. Humira is also given, this is crazy to read another case with pretty much exact same symptoms... she’s been dealing with this for over 2 years now unfortunately
Margarine used to be almost entirely hydrogenated vegetable oil as I recall. When I gave up sugar in the mid-1980s I also gave up all hydrogenated oils. It used to be hard to find snacks back then, but it's gotten easier in the last 10 years or so with the info coming out about trans-fats.
So it could be in your food, and you wouldn’t know it without reading the ingredients label. If you only ate it once this probably wouldn’t be a concern.

") .
.