

Julie Gardener
New Member
1955 - ACTA UNIVERSITATIS PALACKIANAE OLOMUCENSIS - TOM. VI.
Prof. Jan Kabelik - HEMP AS A MEDICAMENT
Importance of hemp seeds in the tuberculosis therapy
INTRODUCTION
During the thirties and forties, in the absence of antibiotics, chemotherapeutics and surgical methods, tuberculosis was rather effectively treated with a therapeutic diet, developed by a team of medical doctors in a sanitarium for patients suffering with tuberculosis at Jince.
The concept was based on two assumptions:
1. ln order to fight tuberculosis effectively, nutrition must supply building material for renewal of tissues destroyed by the disease, be it lungs, other organs, or muscles.
2. The whole diet must support effective function of the liver, thus assuring proper assimilation and utilization of nutrients.
In addition to the selection of nutritious and well-balanced dietary components, attention was paid to the preparation of the food; namely assuring that the nutrients would not be denaturalized. coagulated or rancid due to improper storage or cooking methods.
Two components were considered most important and irreplaceable in the whole diet: oat flakes and a specially processed extract of hemp seed.
It was hemp seed, which attracted the author's attention. It is high in protein (33.0%) and its main protein type, edestine, is well known for its wealth of enzymes and unusual amino acid composition. Most valuable is the amino acid arginin, which is considered essential for formation and growth of new tissue.
While other sources of plant protein, for instance soybean protein, contain 6.8% of arginin, edestin contains approximately 3 times as much arginin - 19.0%. This property is of great importance in balancing of diets, requiring high level of arginin.
Before nationalization of the Czechoslovakian Pharmaceutical Industry in 1948, an extract of hemp seed, EDEZYME. was available on the market. Today it is produced as a "home remedv" according to a following recipe:
Ground hemp seed is mixed with warm milk (60 to 80 degrees C) andmaintained at this temperature for at least half an hour. Keeping the product in a water bath, while constantly mixing, prevents coagulation of edestin on the bottom of the container.
Finished product must be pressed and filtered to separate the indigestible and irritating outer layer of seeds from the colloid solution. One dose prepared from 3/8 of a liter of milk and 50 to 80 grams of hemp seed should be consumed by the patient every second day.
Inclusion of EDEZYM, oat flakes and other, more common dietary components, was tested on two groups of children suffering from tuberculosis in both prewar and war periods. Though no other medication was used and food was rather scarce, all children were considered successfully treated or improved at the end of treatment period. Dietary and/or medical properties of hemp seed deserve our full attention.
I.
If we are discussing the use of hemp seed in the therapy of tuberculosis, we don't think about chemotherapy in today's sense of the word, not even the treatment specifically directed against the Koch bacillus and not a treatment oriented towards diseases that cause changes in the lungs. We think of a total conservative treatment with the emphases on its dietetic or therapeutic nutrition. Therapeutic nutrition becomes then a branch of therapy, namely as a part of the overall effort to "treat the whole human being". For this reason we, according to the Soviet example, begin to understand the importance of the treatment through nutrition in therapy, not excluding physiotherapy. These are, however, the beginnings, lacking direction and therefore up to this point, not too fruitful. One should not be, however, surprised. Even in the Soviet Union the whole question of treatment through nutrition is still controversial, and even the most important nutritional work of the Pevzner school has been subjected to a very critical assessment. Although it was primarily M.I. Pevzner and out of other Soviet authors namely L. M. Model who also in conjunction with tuberculosis rightfully stressed the most important elements of the treatment through nutrition. Another Soviet author, O. L. Gordon, in his presumation entitled "Justification of treatment through nutrition in the clinic and prospects for its expansion" said the following: "Treatment through nutrition is a therapeutic method. As a part of complex therapy it has two goals: To satisfy the physiological needs of the sick organism and to actively influence the pathological process. In this aspect the treatment through nutrition differs from the ordinary nutrition of a sick person". F.K. Mensikov coworker of the Clinic for treatment through nutrition, added that during complex therapy of all diseases proper nutrition is a primary need, while a nutrition which does not take into account the status of the patient could have a negative effect. "Particularly, the treatment through nutrition has an important effect in situations where we need to support regeneration of the tissues, namely when we don't have a medication which could actively support such process". (Presented on December 10, 1954, at the occasion of a scientific conference at Palacky University at Olomouc, as a part of the topic "Hemp seed as a treatment").
It would not be correct to talk about "treatment through nutrition" and not expect from it more than just mere nutrition or doubt that it may actively contribute in the sense of treatment. Even today's physiotherapy, though it has at its disposal rather effective means, can't ignore that such means can be used only for particular patients, and even here one can't put all one's eggs into one basket. In this connection we should remember the words of V.L. Ejnis, used in conclusion of his article 'The work of l. P. Pavlov and clinics of tuberculosis':
"Despite the significant successes of chemotherapy, antibiotics and surgical treatment which substantially improved the prospects of physiotherapy, the fundamental basis of the treatment is still systematic care leading to an increase in the overall resistance of the body. It is now also an important task to improve hygenic-dietetic therapy, incorporating the nutrition of the patient, suffering from tuberculosis".
II.
Towards the end of the first world war physiotherapy freed itself from it helpless position and began a successful attack against tuberculosis. Artificial pneumothorax, exairesa frenicu thoracocaustics, thorakoplatics, extrapleural pneumothorax, Streptomycin, chemotherapy, lobotomy, those are some of the stops on this victorious journey. They are also unquestionable, partial successes, each of which went through a period of excessive hopes and to a point, each of them contributed to the fact that we have forgotten at least partly, the concept of the "Whole human". It leads to a certain indifference to the physiological points of view, hygienic-dietetic treatment, which was critiqued by V.L. Ejnis. The hygienic-dietetic treatment was, by some quiet agreement, reserved for cases, where, for various reasons it was impossible or was not indicated to use "active" means of therapy.
ln the mutual competition for the development of new means of 'active" therapy, our small and in every way, poorly equipped sanitarium at Jince, had only minimum opportunity to participate. The role of Cinderella, however, had some advantages. The less we have been in a position to keep pace with the modern physiotherapy, the more we have concentrated on areas, which were ignored by others. In our small sanitarium we have been in a better position than in other, bigger institutes, to concentrate on hygienic-dietetic treatment, formats the medical nutrition. We have done it correctly. And today, with thirty years of experience behind us, we feel gratified that the Soviet science gradually confirms nearly everything that we have found, be it empirically, by induction or by a series of trials. In perfect function of the liver we have seen a key to the perfect assimilation of nutrients; the first order of the day in our medical nutrition was the following: Exclude or limit to the maximum, food which will burden the liver or in some cases, cause damage to the liver. In nutrition of the patients with tuberculosis put emphasis on components which will protect the liver and enable their smooth function. This way, we actually developed a "liver diet" sooner, more or less coincidentally. We laid the foundation, which became a logical pre-condition of every dietetic effort. The role of the liver for the nutrition of a human, and a sick one in particular, is in its variability so immensely important, that it must be recognized by everyone who would like to maintain the "whole human" in good health, or enable him to recover from whatever sickness.
In keeping with this principle, we have concentrated on excluding or reducing from the nutrition of our patients, less valuable fats, namely rancid or burned, all fried, roasted foods, pork drippings or boiled butter, all meats preserved by salt and canning, all smoked sausages, beef and duck meat, duck eggs and spicy foods. On the other hand, we have emphasized the diet of our patients, a relative surplus of proteins, in the form of light types of meat, dietetically processed, cottage cheese, which was specifically processed to avoid coagulation and denaturalization. sour milk. yogurt, raw egg yolks or only partially boiled to avoid coagulation. Out of fats we recommended only natural fresh butter, fresh cream, olive oil without signs of rancidity, fresh or preserved fruit without any artificial preservatives, imported fruits from the south in fresh or dry form, nuts and almonds. Out of vitamins we recommend plentiful levels of vitamins B1, A and C. We will use potatoes as a side dish but fewer flour based side dishes. boiled vegetables or vegetables steamed with butter, or if possible, raw (carrots). Use few desserts, but of good quality.
With this diet, we have incorporated into the nutrition of our patients, important substances, contained in non-denaturalized fresh fats and proteins and known as liver protecting components (methionine, choline, insitol, unsaturated short chain fatty acids) and amino acids, which are considered metabolically most valuable (methionine, tryptophan. tyrosine. fenylalanine and others). Lastly, we are adding substances, without which the liver can't properly function (thiamin, carotine, ascorbic acid, vitamin F).
This regimen, aimed at liver protection, was combined with a reduction of the daily meals to three, at most four, with 4-5 hours intervals without any food or drink. This also lead to the elimination of over burdening the liver,sometimes blamed on the frequent presentation of food.
These dietetic provisions were practiced in Jince a quarter century ago, and represented at that time, and even now, a courageous deviation from common practice. Similarly, a suggestion of Prof. Arnerling, from Olomouc, requesting that the nutrition of patients, suffering with tuberculosis. must fully respect the function of the liver, was an expiring voice in the desert. Only long-term effort and undying persistence enabled us to keep such reforms alive and viable until the time, when the Soviet science on "medical nutrition' demonstrated their competency.
III.
The value of the tree can be judged by the fruit. The value of the medical nutrition by the nutritional and medical results. If we value individual nutritive components during the systematic nutritional and medical trials using such criteria, we would soon find out the importance of the correct selection of particular proteins as well as their state and preparation. Though meat is the most common source of protein and its importance in nutrition is beyond an argument, in medical nutrition, it's importance is far behind the proteins in milk and eggs. Eggs represent exclusive building material of the bird's embryo, while milk is a primary source of nutrients in quickly growing and well prospering young mammals. I think that we rightfully call these proteins "plastic", as they are the true material from which the body tissues are built.
A daily intake of 100-150 grams of specially prepared loose cottage cheese in the state of hydrogel, and two egg yolks mixed together with other components of the diet, will have much more positive effect on the health status of a sick person than their weight or caloric equivalent in the form of meat. We can't however, expect such effects in a cottage cheese which is coagulated, denaturalized, or prepared by quick coagulation of milk which was too acidic and brought to too high temperature. Similarly, the egg yolk must not be coagulated by boiling to a "hard" state or by frying or other inappropriate preparation methods.
With diseases, such as tuberculosis, which in its active stage is characterized by its tendency for destruction of not only the affected organ (lungs), but as well of the whole body (loss of weight, autolysis of muscles and other tissues, we can't value enough such food, which can serve the living organism as building material. As well, we must present this rare material to the patient's organism in a natural colloid state in which the specific dynamic effect will be best preserved.
The importance of this premise will be more obvious if we, in addition to proteins of animal origin, include proteins of vegetable origin. The main sources of vegetable proteins, suitable for the nutrition of human are seeds, grains and other fruits. Some can be eaten in a raw state, fresh or professionally dried (nuts or figs); in this later case we should not worry about denaturalization. Unfortunately. the majority of people depend for their nutrition on cooked and baked foods, made out of meal. The aleurone layer of the cereal grains, containing dietetically important proteins and rich in vitamin B1 will remain in the mill. The rest is denatualized by baking or boiling in water. It is hard to believe that professionally prepared oat flakes, in a dose of 15-20 grams will affect the distinct restitution of nutritional status and stimulate healing processes. On the other hand, a ten to twenty times higher dose of cereal proteins in denaturalized and coagulated state, will have no effect in this area. There are, however, certain differences between oats and other cereal grains.
In oats, the aleurone layer is preserved. In addition to vitamin B1, oats contain vitamin B2 in larger quantities than other cereal grains. In its protein structure, the gliadin form dominates over glutenin; the fat content is much higher, giving the oat flake a hazelnut flavor and contributing to the elimination of hunger. The content of gluconins, components which lower the blood sugar, has the same effect "per se" as insulin has when applied parenterally. The majority of the strong points of oats are wasted if oat flakes are boiled in water or in soup, or denaturalized by other improper method. What will be left is just a food, rich in calories but without the medicalnutritional effects. Only the milk and careful preparation will keep the proteins of oat grains in colloid and dietetically active state.
IV.
From the oat grain there was a direct route to the hemp seed or "semenec". Not perhaps because our forefathers considered hemp seed porridge and soup as "not bad food", but because by its content of edestin and a wealth of enzymes, hemp seed ranks among the best seeds overall.
Chemically, edestin differs substantially from gliadin and other cereal proteins. It is closer to the proteins of nuts and oil seeds and contains a high amount of arginin (up to 19%), which is the amino acid that encourages growth and formation of new tissues. Similarly, as in casein it contains methionine, which is known for its protective function of the liver. As casein, it contains tryptophan (important provitamin pp-niacine), which is missing in cereals and without which it is impossible to achieve a nitrogen balance. It contains nearly all known amino acids, namely the essential ones, without which the growth and well being of the organism is impossible. Without it, food could never be complete and hvpoproteminaemy occurs - an event, singled out the by Soviet author L.M. Model as the root of the disease of tuberculosis. It is impossible in this short presentation to go into greater detail. Let's, however, bear in mind that the amino acids, which are the most important in the medical nutrition - tryptophan, tyrosinc, phenylalaninc - are separated during the digestion of edestin first. Furthermore, the arginin, cystein and alaninc content in edestin is much higher than in other proteins of plant or animal origin. Finally, amino acids, which are in edestin in smaller quantity than in proteins of animal origin, can be easily replaced in medical nutrition by cottage cheese. There are plenty of reasons why hemp seed edestin should be, in addition to cottage cheese, egg yolk and oat gluten, included among the most important components of medical nutrition for patients with tuberculosis.
As we have witnessed in conjunction with the other proteins, it is of great importance, particularly in the case of edestin, to maintain it in colloid state. From this point of view, our product EDEZYM (the name originated from two words: edestin and enzyme), was very suitable. It has been available on the market for a number of years, though was discontinued after the nationalization of the pharmaceutical industry, in 1948. We may use, however, a simple home preparation, assuming that we have a high quality hemp seed, no older than two years, in which all the proteins and enzymes are still fully active (in order to find out we may conduct a germination test). Old recipes, in which our forefathers prepared the hemp seed soup or porridge, are not useful anymore. In the majority of cases, they lead to coagulation and denaturalization of edestin. ln the preparatory stage we have to remove the outside layer of the seed, which in contrast to oats, is indigestible, discourages the intake and is irritating during the digestion. The only remaining solution is to transfer the content of the seed into a colloid solution and remove the indigestible residue by pressing and sifting.
The best method is based on the extraction of ground hemp seeds by hot milk (60-80 degrees C). The content is constantly mixed while it is kept in a water bath (double boiler), which prevents the excessive heating of the bottom of the container. If this is not done properly, edestin starts to coagulate from the bottom. Sometimes it fully coagulates. Milk could be skimmed, but must be fully fresh and without preservatives. Sweet whey may be used as well. We can obtain it by the coagulation of casein with chymosine. Maceration of the hemp seed, at the above mentioned temperature. should last at least half an hour, preferably more. The finished colloid must be aggressively pressed, filtrated, in some cases mildly sweetened and offered to the patient either immediately or kept at a temperature of 60 degrees C in a water bath, until used. This will prevent hydrolics or fermentative breakdown of the active components. One dose, prepared from 3/8 litre of milk and 50-80 grams of hemp seed, should be consumed by the patient every second day on an empty stomach.
V.
The human organism is capable of dealing, under favourable conditions and to a certain level, with the tuberculosis illness without particular treatment. During times, when calmetisation was unknown and modern antibiotics and tuberculostatics were not available, the majority of primary effect cases were healed spontaneously, at least as far as children beyond the baby stage are concerned. Certainly, the modern organization of the fight against tuberculosis (calmetization, the introduction of child preventative medicine, regular Rig check-ups) lead to a significant reduction in small children morality and proving that we can't rely too much, or exclusively, on the spontaneous healing and protective properties of the child's organism.
This is more true in cases of post primary (secondary) child tuberculosis of lungs and Iymphatic glands. Here, as well, we can see a significant tendency for spontaneous healing, but the assumption of favorable conditions plays a decisive role. lt was for this reason, that during the not so distant past, the cases of "secondary" lung tuberculosis, prevalent in children of school age,the mortality level was rather high, namely among poor people.
This fact underlies again the importance of living conditions. In mature individuals (therial lung pthisis), though the spontaneous healing of lung damage is much rarer than in children, it is much more probable where the living conditions are more favourable. lt is for this reason, that a higher percentage of mature people were saved from the upper layers of the society.
lt is true, however, that wealth and poverty must not necessarily synonymous with good and bad living conditions. But, in contrast to the present days when living conditions in our countrv are more or less uniformly provided, wealthy people were able to assure for themselves favourable living conditions, assuming they understood what represents "true favourable living conditions". Money without knowledge is not enough. The knowledge, which is required, is defined in every time period by the scientific content of the term "hygienic-dietetic healing".
The substance of this "term" developed historically, is changing constantly and will, in conjunction with the general scientific development, continue to change always. It was not a long time ago, when overfeeding a patient suffering from tuberculosis, without taking into consideration the effect on the liver function, was considered purposeful and desirable. Today we have corrected many things, however, many more cry for change. The fast and successful development of "active" treatment methods seems to absorb excessively the attention of ftisoclogs and this leads to insufficient interest in systematic improvements and scientific involvement in hygienic-dietetic methods. This is happening at times when nobody denies that even the most effective "active methods" must be supported by hygienic-dietetic methods, the necessary foundation of all anti-tuberculosis treatments.
Why, then, despite all the progress in "active" therapy, do the hygienic-dietetic methods (foremost the medical nutrition) remain the necessary foundation of all treatments? Why from those methods (and specifically from them) do we expect the fulfillment of the favourable conditions, which make the treatment much easier, and which in some cases, make spontaneous healing possible?
To generate or restore such conditions, during which the human organism is capable of dealing successfully with the disease, is the main mission of hygienic-dietetic treatment and specifically the medical nutrition. lf we are successful and wish to call the resulting healing process "spontaneous" it is only a question of suitable terminology.
If; by using the certain system of medical nutrition, we achieve, in the treatment of tuberculosis, spontaneous healing with considerable probability or regularity, and if we, at the same time. achieve a restitution of the overall nutritional state, during which the tuberculosis slowed down and decreased, then we have solved our problem. This means that we have found the favourable conditions, under which the human organism can better resist the tuberculosis, or deal with it successfully.
VI.
As a testing stone of such systems of medical nutrition, we can best use the cases of post primary (secondary) child tuberculosis of lymphatic glands and lungs, accompanied by substantial degradation of total nutritional status of body development. Such cases tend to show a substantial tendency towards "spontaneous healing', assuming that the living conditions are favorable. If we can achieve, in such cases, dramatically favourable turns for the better as far as the healing of the lung damage and as far as the nutritional status and body development is concerned, then we have, with the highest probability, presented a proof that the system we have used represents the "favorable conditions".
In the following part, I present two groups of children which will offer the necessary documentation for this case.
The first group of 16 children (8 boys and 8 girls) was treated in Jince sanitarium in 1938. In this difficult period, when the sanitarium - at that time a private enterprise - was, because of the world's economic crises, basically idling. Faced with the threat of Hitler's occupation, I have offered the Red Cross in Prague an expense free stay and treatment for 20 children with tuberculosis. In a few days we filled the first floor of the building by these, exceptionally welcomed guests, sick members of Prague's poor from the following districts: Nusle, Pankrac, Michle, Kosire and Kobylisy. After a few days we excluded four of the 20 children and returned them back to Prague. Two were excluded because we did not diagnose any active tuberculosis changes and two others for other reasons. The remaining 16 children remained under treatment for various lengths of time, as is discussed later.
The children came to us in a state of more or less depressed nutrition. The tuberculosis (primary and secondary) was confirmed and checked by the Prague doctors, from whom we received the children.
While with us, the children (as well as the mature patients) were offered meals three times a day. They drank only during the meal. There could be no doubt that they were not overfed. Once a day, they had the main meal, based on meat. once a day they received 100 g of cottage cheese, 25 g of cream (in Czech: "rozhuda"). Once a day they were offered oat porridge made from 15 g of oat flakes. At noon, always after they consumed soup, they received 75 g of shredded carrots with few drops of lemon juice and a soup spoon of cream. Twice a day they received 100 grams of fruit, twice a day 20 g of fresh butter from a farm. Otherwise they received mixed home meals with one limitation. All foods, which would have excessively burdened the liver, were excluded.
The children did not use any other medication, with the exception of colloidal extract of hemp seed. EDEZYM, which was described in part IV. Three times a day the children received soup spoon of Edezym, always a quarter hour before the meal (without a drink), then vitamin B1 and vitamin C. They received two tablets daily, though the food was rather vitamin rich.
The lack of appetite and fussiness toward food, characteristic in children suffering with tuberculosis, was gone in all children, without exception, during the first days of treatment. We also noticed in all children from the first days, a distinct and pervasive change in the total health status.
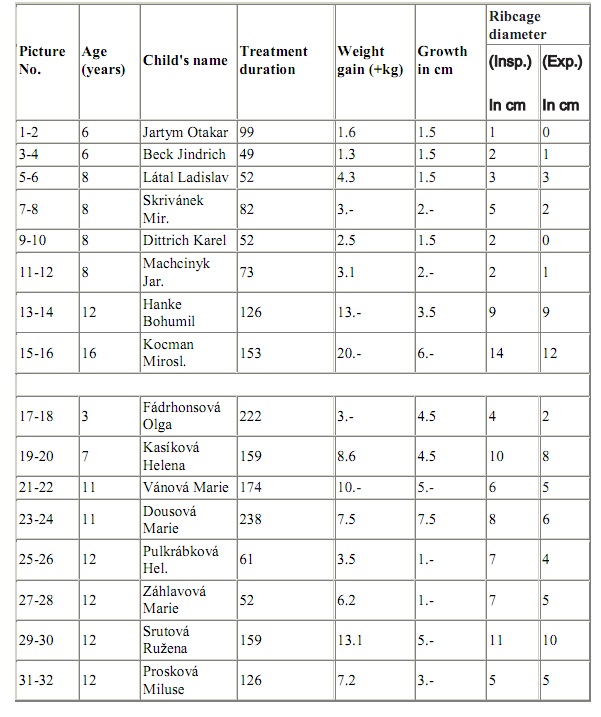
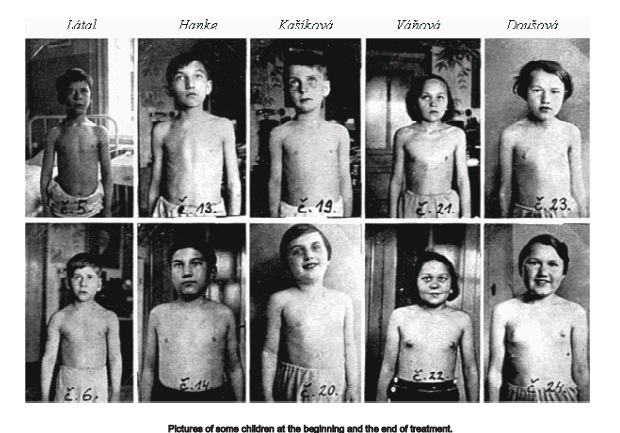
The boys gained on average 1 kg. within 14 days; girls within 20 days. Boys increased their height by 1 cm in 35 days, girls in 38 days. The diameter of the rib cage was increasing in boys by 1 cm in 18 days, while in girls in 20 days. This improvement in the total physical state and body development in all 16 children is obvious from the pictures, made at the beginning of the treatment. Together with the data, collected from individual children, they are presented in the following overview:
Since the whole group of 16 children were treated at the same time and by the same method, with results indisputably positive there is no doubt. that the treatment was effective. The food, offered three times a day, was neither more abundant or calorically richer than the one which was offered in other institutions and in a majority of families where a child was identified as sick and in need of substantial nutrition. On the contrary, at those institutions we could talk about overfeeding, where meals are presented five or six times a day and the caloric value is higher.
The calories on the plate are not helping if we can't formulate the diet in such a way that the nutrients are utilized and assimilated. Our approach can be summarized in three parts:
1. Preventing overburdening of the liver and other digestive and metabolic organs with harmful foods, offered too frequently. We are trying to encourage their proper functioning by offering some ingredient with specific properties (vitamins and others).
2. We are offering, if possible at every meal, some of the "plastic" proteins, which we have recognized as being natural building material, essential for the formation of animal and plant organisms (cottage cheese, egg yolk, reserve proteins from various plant products, cereal and specifically oat gluten, edestin from hemp seed).
3. Such "plastic" proteins are offered in seemingly small daily doses (for instance 100 g of cottage cheese, I yolk, a few nuts, barely 15 to 20 grams of oats and same amount of hemp seed) but in colloid form, not denaturalized and not coagulated.
The importance of such modified and with hemp seed edestin supplemented medical nutrition will be even more obvious, when we realize, that it was the only substantive base of the whole treatment. During this medical nutrition, we have supplemented the diet with EDEZYM, and not used other medication or medical treatment. ln 1932, other effective medications against tuberculosis were not even available.
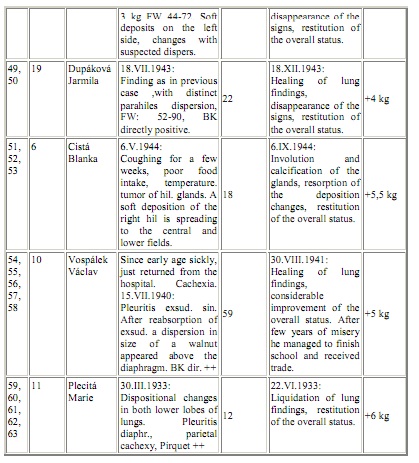
The other 10 cases represent a looser group of children and teenagers who were treated during the second world war - during the occupation. Only one case took place earlier, in 1933, and this girl (11 year old Maria Plecita) was included to this group as, with exception of the time the treatment took place, all the other factors (pathology, therapy) were the same as for the remaining 9 children in the group.
During this period the sanitarium was fully occupied by mature patients, only five years old Ludek Ledecky undertook the treatment together with his father, suffering with tuberculosis as well. Others were treated at home, under our ambulant supervision. Even this group does not represent specific selection, it included all children we have ambulantly treated. They were considered altogether exceptional.
The level of the nation's nutrition during this period was not good and the children under the home regimen were missing many things, which the sanitarium had in abundance for the children in the first group, in 1938. There was no cream. The cottage cheese was also in short supply and when the parents of the small patients were able to acquire it, the quality was low, as it was hard and coagulated. There was a shortage of butter and high quality fats in general. Similarly, quality meat and sometimes even eggs, sugar and other important food ingredients were not available. Such nutrition was inadequate even for healthy people but even more so for the sick ones. This hard time, however, left our patient two things, which, in addition to cottage cheese, were perhaps the most important: oat flakes and EDEZYM. Consequently, we have been able, during this difficult period and with half way correct home diet, to achieve with this second group of children convincing nutritional and treatment results, equal to the ones achieved in 1938.
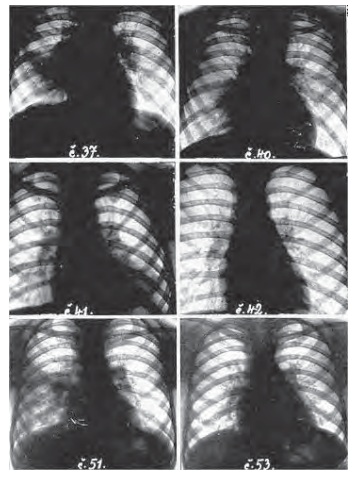
These cases. which were part of the second group, took place when the children were not even protected by "calmetisation" or could have been saved by chemotherapy, or by antibiotics. It is obvious as well, that at that time, we didn't have at our disposal detailed diagnostic analysis of individual cases, which would satisfy today's requirements of phthisiology. In particular, we did not have the tomographic data and so we have only estimated, using X-ray pictures, where the atelectasc ends and the inflammation changes begin, when and to what extent we can demonstrate break up and where the dissemination took place. Nevertheless, even this norrnal skiagram brings sufficiently convincing evidence, that to all children in this group, the treatment brought about a significant turn over in the disease, which was, up to this point, considered "progressive". This means that it brought about a regression of the pathological changes in glands and lungs and, in the majority, also a distinct "restitution and integrum". If we add to it that paralicly with the positive development of the lung finding. We have seen in all children, right from the beginning, a similarly positive change in the total health status, which had, before the treatment started, deteriorated progressively. It was clear that to bring about full curative and nutritional effects, even the little which remained available from our medical nutrition during this war period (oat meal, hemp seed, a little cheese, a few yolks, and protection of the liver) was sufficient and that in this "little" is the substance of the effective factor.
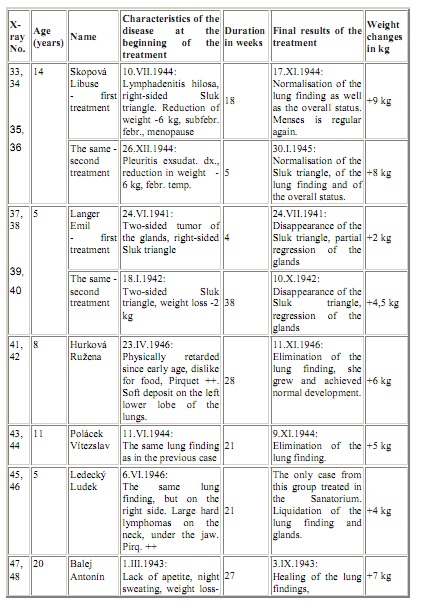
In the following table, we have summarized the curative effects. which were achieved by the treatment of the second group of ten ambulantly treated children. The summary deals with the effects of lung findings and the total nutritional state and development:
On a group of twenty-six tuberculosis stricken children and teenagers, presented in two groups in "as the herd is running" fashion (this means without any selection), we have been able to achieve positive results. From the point of treatment, nutrition, or physical development, medical nutrition, supplemented with the hemp seed edestin, had an unambiguously favorable effect.
The attached documentation, generated ten to twenty years of age, will not meet today's requirements of the phthisiology. It leaves in some cases doubts if the described type of pathological change or group of changes was or was not of the specific type. There is, however. not a slightest doubt about the following:
1. All children were included into our treatment program in the state of progressive worsening of total health status and also in the majority of cases with documented lung disease;
2. In all participants this treatment immediately caused a turn over in the sense of regression of changes caused by the disease and improvement of the overall health status;
3. In all cases, without any other medication or treatment procedures, within a usually short time, a healing of the lung or glands disease was accomplished. And, during the same short period of time, with only three meals a day, not excessively rich, a farreaching restitution of the nutritional status and physical development was noticed.
Out of these facts it is obvious that this treatment of medical nutrition proved to be good and very effective. It was happening in a time period when similarly effective means of treatment were not available. In this sense, the treatment was saving the lives of children threatened by tuberculosis (as well as mature people) and was in a position to save many more if it only received the deserved attention.
In the first group of 16 children belonging to the poor people of the Prague suburb, somebody may have commented,that the turn over in their health status was influenced by removing these children from unhealthy living conditions and housing them in a hygienic and rather "affluent environment". It could not be denied that this was an important factor, which had a positive influence, it has an effect during each transfer of a sick child into a hospital, however, we don't see in every case such a change. We do not see such a straight forward means. As well, this objection loses it merit when we compare the first group of children with the second group which, with only one exception, did not changed their environment, but were treated at home.
Moreover, this relatively "affluent environment" was often restricted by the miserable economic condition during the war. Despite that, in such unfavorable conditions, we witness the same convincing and unambiguous results, the same overall improvement.
It is exactly this comparison of the two groups of children which leads us to the discovery of the factors which were effective in the treatment of both groups. For certainly, it was not the effect of the changed environment and "comparative affluence" which we provided for the children in the first group, but which was not available for the children in the second group. It must have been the parts of the treatment which were available to both groups. From the effective substances we should name: porridge from the oat flakes, EDEZYM from the hemp seeds, and cottage cheese. Further, we should add the protection of the liver, which means the exclusion of meals which are overburdening the liver and the exclusion of frequent presentations of meals and drinks.
If we take the preservation of liver as a logical part of the patient's hygiene, we can condense the whole topic to three factors: oatmeal porridge, EDEZYM and cottage cheese. It is not to say that raw or "soft" egg yolk, nuts, raw vegetables and fruits and other, previously discussed things are not important. But the most important, as we can conclude from our analysis, are the three: oats, hemp seed and cottage cheese. And, we repeat, that all three must be prepared in such a way that the proteins will be colloid, under-naturalized and in a non-coagulated state. All other effective substances of the medical nutrition could be, more or less, missed by the patient, as they were missed by the children in the second group, without endangering the results of the medical nutrition. If, however, one of the three basic pillars of the treatment is missing, or is damaged (denaturalized) by the improper processing, the results of the treatment are half as effective or less effective.
Today, when we don't have EDEZYM and the cottage cheese is sometimes of poor quality, we have Streptomycin, PAS, and INH, in addition to surgical methods. Let's be careful, however! A conscientious doctor always considers the strong points and weaknesses of such medications and while treating the mature patients, or even more, while treating the children, he uses them only in cases where they are needed and in doses which are tolerable. If he understands the importance of liver protection, he is twice as careful, particularly when dealing with para-aminosalicylic acid. And makes sure "that he will not use all his ammunition before the main battle starts". This means he avoids the frivolous use of full doses of antibiotics and bacteriostatical drugs, so that in case of exacerbation or recidivity, he will not be without an effective weapon. All such unavoidable considerations must reinforce our conviction, that a means which is relatively effective and at the same time absolutely harmless when used for an extended and unlimited period, as is our medical nutrition, should not be overlooked even today, in a time of antibiotics.
We, in Jince, even today subject our patients, who are mature and chronic, to the appropriate preparation before we will use antibiotics or tuberculostatics. Those who need it, will be educated in the proper order in eating and drinking. Smokers are retrained into non-smokers and all are included into a regimen of liver protection. Usually, we achieve, particularly in disciplined patients, a nice improvement, without medication. Only in cases when the treatment progress is slow, do we, after careful consideration, use antibiotics and bacteriostatics. Patients will, however, always be supported by medical nutrition. This medical nutrition is an essential part of our patient's education while they are being treated at home.
SUMMARY
The use of hemp seed in the therapy of tuberculosis is based on our experience of the last thirty years, gained at Jince in the area of medical nutrition. In the proper function of the liver we have always seen a precondition for perfect assimilation of nutrients. For this reason we have emphasized the rules and limitations which we know today as the foundation of liver diet. We consider them to a certain point as a universal base of every medical diet. Medical nutrition during tuberculosis must stress, in addition to vitamins B1, C and A, primarily proteins and among them namely those which nature destined to serve as building material for the formation of organisms. Such protein sources, for instance, include cottage cheese, egg yolk, reserve proteins in cereals, nuts and other fruits. It is of great importance. that such proteins are processed without denaturalization. Professionally prepared cottage cheese is a precious dietetic component, but hard and coagulated is dietetically worthless. Similarly, raw egg yolk is a good, but boiled to hard state is not. A daily does of only 10 to 20 grams of oats, in the form of professionally prepared porridge will soon prove its medicinal properties, while twenty times higher doses of cereals denaturalized by baking or cooking in water have a dietetically rather indifferent affect. The ground hemp seed, extracted with milk, heated to a temperature between 60 to 80 degrees C will have, even in such small doses, an important healing effect. We are convinced that a child with tuberculosis is the best testing ground for medical nutrition based on hemp seed.
Source: hemphearts.com/HempHeartsStudy.pdf
Prof. Jan Kabelik - HEMP AS A MEDICAMENT
Importance of hemp seeds in the tuberculosis therapy
INTRODUCTION
During the thirties and forties, in the absence of antibiotics, chemotherapeutics and surgical methods, tuberculosis was rather effectively treated with a therapeutic diet, developed by a team of medical doctors in a sanitarium for patients suffering with tuberculosis at Jince.
The concept was based on two assumptions:
1. ln order to fight tuberculosis effectively, nutrition must supply building material for renewal of tissues destroyed by the disease, be it lungs, other organs, or muscles.
2. The whole diet must support effective function of the liver, thus assuring proper assimilation and utilization of nutrients.
In addition to the selection of nutritious and well-balanced dietary components, attention was paid to the preparation of the food; namely assuring that the nutrients would not be denaturalized. coagulated or rancid due to improper storage or cooking methods.
Two components were considered most important and irreplaceable in the whole diet: oat flakes and a specially processed extract of hemp seed.
It was hemp seed, which attracted the author's attention. It is high in protein (33.0%) and its main protein type, edestine, is well known for its wealth of enzymes and unusual amino acid composition. Most valuable is the amino acid arginin, which is considered essential for formation and growth of new tissue.
While other sources of plant protein, for instance soybean protein, contain 6.8% of arginin, edestin contains approximately 3 times as much arginin - 19.0%. This property is of great importance in balancing of diets, requiring high level of arginin.
Before nationalization of the Czechoslovakian Pharmaceutical Industry in 1948, an extract of hemp seed, EDEZYME. was available on the market. Today it is produced as a "home remedv" according to a following recipe:
Ground hemp seed is mixed with warm milk (60 to 80 degrees C) andmaintained at this temperature for at least half an hour. Keeping the product in a water bath, while constantly mixing, prevents coagulation of edestin on the bottom of the container.
Finished product must be pressed and filtered to separate the indigestible and irritating outer layer of seeds from the colloid solution. One dose prepared from 3/8 of a liter of milk and 50 to 80 grams of hemp seed should be consumed by the patient every second day.
Inclusion of EDEZYM, oat flakes and other, more common dietary components, was tested on two groups of children suffering from tuberculosis in both prewar and war periods. Though no other medication was used and food was rather scarce, all children were considered successfully treated or improved at the end of treatment period. Dietary and/or medical properties of hemp seed deserve our full attention.
I.
If we are discussing the use of hemp seed in the therapy of tuberculosis, we don't think about chemotherapy in today's sense of the word, not even the treatment specifically directed against the Koch bacillus and not a treatment oriented towards diseases that cause changes in the lungs. We think of a total conservative treatment with the emphases on its dietetic or therapeutic nutrition. Therapeutic nutrition becomes then a branch of therapy, namely as a part of the overall effort to "treat the whole human being". For this reason we, according to the Soviet example, begin to understand the importance of the treatment through nutrition in therapy, not excluding physiotherapy. These are, however, the beginnings, lacking direction and therefore up to this point, not too fruitful. One should not be, however, surprised. Even in the Soviet Union the whole question of treatment through nutrition is still controversial, and even the most important nutritional work of the Pevzner school has been subjected to a very critical assessment. Although it was primarily M.I. Pevzner and out of other Soviet authors namely L. M. Model who also in conjunction with tuberculosis rightfully stressed the most important elements of the treatment through nutrition. Another Soviet author, O. L. Gordon, in his presumation entitled "Justification of treatment through nutrition in the clinic and prospects for its expansion" said the following: "Treatment through nutrition is a therapeutic method. As a part of complex therapy it has two goals: To satisfy the physiological needs of the sick organism and to actively influence the pathological process. In this aspect the treatment through nutrition differs from the ordinary nutrition of a sick person". F.K. Mensikov coworker of the Clinic for treatment through nutrition, added that during complex therapy of all diseases proper nutrition is a primary need, while a nutrition which does not take into account the status of the patient could have a negative effect. "Particularly, the treatment through nutrition has an important effect in situations where we need to support regeneration of the tissues, namely when we don't have a medication which could actively support such process". (Presented on December 10, 1954, at the occasion of a scientific conference at Palacky University at Olomouc, as a part of the topic "Hemp seed as a treatment").
It would not be correct to talk about "treatment through nutrition" and not expect from it more than just mere nutrition or doubt that it may actively contribute in the sense of treatment. Even today's physiotherapy, though it has at its disposal rather effective means, can't ignore that such means can be used only for particular patients, and even here one can't put all one's eggs into one basket. In this connection we should remember the words of V.L. Ejnis, used in conclusion of his article 'The work of l. P. Pavlov and clinics of tuberculosis':
"Despite the significant successes of chemotherapy, antibiotics and surgical treatment which substantially improved the prospects of physiotherapy, the fundamental basis of the treatment is still systematic care leading to an increase in the overall resistance of the body. It is now also an important task to improve hygenic-dietetic therapy, incorporating the nutrition of the patient, suffering from tuberculosis".
II.
Towards the end of the first world war physiotherapy freed itself from it helpless position and began a successful attack against tuberculosis. Artificial pneumothorax, exairesa frenicu thoracocaustics, thorakoplatics, extrapleural pneumothorax, Streptomycin, chemotherapy, lobotomy, those are some of the stops on this victorious journey. They are also unquestionable, partial successes, each of which went through a period of excessive hopes and to a point, each of them contributed to the fact that we have forgotten at least partly, the concept of the "Whole human". It leads to a certain indifference to the physiological points of view, hygienic-dietetic treatment, which was critiqued by V.L. Ejnis. The hygienic-dietetic treatment was, by some quiet agreement, reserved for cases, where, for various reasons it was impossible or was not indicated to use "active" means of therapy.
ln the mutual competition for the development of new means of 'active" therapy, our small and in every way, poorly equipped sanitarium at Jince, had only minimum opportunity to participate. The role of Cinderella, however, had some advantages. The less we have been in a position to keep pace with the modern physiotherapy, the more we have concentrated on areas, which were ignored by others. In our small sanitarium we have been in a better position than in other, bigger institutes, to concentrate on hygienic-dietetic treatment, formats the medical nutrition. We have done it correctly. And today, with thirty years of experience behind us, we feel gratified that the Soviet science gradually confirms nearly everything that we have found, be it empirically, by induction or by a series of trials. In perfect function of the liver we have seen a key to the perfect assimilation of nutrients; the first order of the day in our medical nutrition was the following: Exclude or limit to the maximum, food which will burden the liver or in some cases, cause damage to the liver. In nutrition of the patients with tuberculosis put emphasis on components which will protect the liver and enable their smooth function. This way, we actually developed a "liver diet" sooner, more or less coincidentally. We laid the foundation, which became a logical pre-condition of every dietetic effort. The role of the liver for the nutrition of a human, and a sick one in particular, is in its variability so immensely important, that it must be recognized by everyone who would like to maintain the "whole human" in good health, or enable him to recover from whatever sickness.
In keeping with this principle, we have concentrated on excluding or reducing from the nutrition of our patients, less valuable fats, namely rancid or burned, all fried, roasted foods, pork drippings or boiled butter, all meats preserved by salt and canning, all smoked sausages, beef and duck meat, duck eggs and spicy foods. On the other hand, we have emphasized the diet of our patients, a relative surplus of proteins, in the form of light types of meat, dietetically processed, cottage cheese, which was specifically processed to avoid coagulation and denaturalization. sour milk. yogurt, raw egg yolks or only partially boiled to avoid coagulation. Out of fats we recommended only natural fresh butter, fresh cream, olive oil without signs of rancidity, fresh or preserved fruit without any artificial preservatives, imported fruits from the south in fresh or dry form, nuts and almonds. Out of vitamins we recommend plentiful levels of vitamins B1, A and C. We will use potatoes as a side dish but fewer flour based side dishes. boiled vegetables or vegetables steamed with butter, or if possible, raw (carrots). Use few desserts, but of good quality.
With this diet, we have incorporated into the nutrition of our patients, important substances, contained in non-denaturalized fresh fats and proteins and known as liver protecting components (methionine, choline, insitol, unsaturated short chain fatty acids) and amino acids, which are considered metabolically most valuable (methionine, tryptophan. tyrosine. fenylalanine and others). Lastly, we are adding substances, without which the liver can't properly function (thiamin, carotine, ascorbic acid, vitamin F).
This regimen, aimed at liver protection, was combined with a reduction of the daily meals to three, at most four, with 4-5 hours intervals without any food or drink. This also lead to the elimination of over burdening the liver,sometimes blamed on the frequent presentation of food.
These dietetic provisions were practiced in Jince a quarter century ago, and represented at that time, and even now, a courageous deviation from common practice. Similarly, a suggestion of Prof. Arnerling, from Olomouc, requesting that the nutrition of patients, suffering with tuberculosis. must fully respect the function of the liver, was an expiring voice in the desert. Only long-term effort and undying persistence enabled us to keep such reforms alive and viable until the time, when the Soviet science on "medical nutrition' demonstrated their competency.
III.
The value of the tree can be judged by the fruit. The value of the medical nutrition by the nutritional and medical results. If we value individual nutritive components during the systematic nutritional and medical trials using such criteria, we would soon find out the importance of the correct selection of particular proteins as well as their state and preparation. Though meat is the most common source of protein and its importance in nutrition is beyond an argument, in medical nutrition, it's importance is far behind the proteins in milk and eggs. Eggs represent exclusive building material of the bird's embryo, while milk is a primary source of nutrients in quickly growing and well prospering young mammals. I think that we rightfully call these proteins "plastic", as they are the true material from which the body tissues are built.
A daily intake of 100-150 grams of specially prepared loose cottage cheese in the state of hydrogel, and two egg yolks mixed together with other components of the diet, will have much more positive effect on the health status of a sick person than their weight or caloric equivalent in the form of meat. We can't however, expect such effects in a cottage cheese which is coagulated, denaturalized, or prepared by quick coagulation of milk which was too acidic and brought to too high temperature. Similarly, the egg yolk must not be coagulated by boiling to a "hard" state or by frying or other inappropriate preparation methods.
With diseases, such as tuberculosis, which in its active stage is characterized by its tendency for destruction of not only the affected organ (lungs), but as well of the whole body (loss of weight, autolysis of muscles and other tissues, we can't value enough such food, which can serve the living organism as building material. As well, we must present this rare material to the patient's organism in a natural colloid state in which the specific dynamic effect will be best preserved.
The importance of this premise will be more obvious if we, in addition to proteins of animal origin, include proteins of vegetable origin. The main sources of vegetable proteins, suitable for the nutrition of human are seeds, grains and other fruits. Some can be eaten in a raw state, fresh or professionally dried (nuts or figs); in this later case we should not worry about denaturalization. Unfortunately. the majority of people depend for their nutrition on cooked and baked foods, made out of meal. The aleurone layer of the cereal grains, containing dietetically important proteins and rich in vitamin B1 will remain in the mill. The rest is denatualized by baking or boiling in water. It is hard to believe that professionally prepared oat flakes, in a dose of 15-20 grams will affect the distinct restitution of nutritional status and stimulate healing processes. On the other hand, a ten to twenty times higher dose of cereal proteins in denaturalized and coagulated state, will have no effect in this area. There are, however, certain differences between oats and other cereal grains.
In oats, the aleurone layer is preserved. In addition to vitamin B1, oats contain vitamin B2 in larger quantities than other cereal grains. In its protein structure, the gliadin form dominates over glutenin; the fat content is much higher, giving the oat flake a hazelnut flavor and contributing to the elimination of hunger. The content of gluconins, components which lower the blood sugar, has the same effect "per se" as insulin has when applied parenterally. The majority of the strong points of oats are wasted if oat flakes are boiled in water or in soup, or denaturalized by other improper method. What will be left is just a food, rich in calories but without the medicalnutritional effects. Only the milk and careful preparation will keep the proteins of oat grains in colloid and dietetically active state.
IV.
From the oat grain there was a direct route to the hemp seed or "semenec". Not perhaps because our forefathers considered hemp seed porridge and soup as "not bad food", but because by its content of edestin and a wealth of enzymes, hemp seed ranks among the best seeds overall.
Chemically, edestin differs substantially from gliadin and other cereal proteins. It is closer to the proteins of nuts and oil seeds and contains a high amount of arginin (up to 19%), which is the amino acid that encourages growth and formation of new tissues. Similarly, as in casein it contains methionine, which is known for its protective function of the liver. As casein, it contains tryptophan (important provitamin pp-niacine), which is missing in cereals and without which it is impossible to achieve a nitrogen balance. It contains nearly all known amino acids, namely the essential ones, without which the growth and well being of the organism is impossible. Without it, food could never be complete and hvpoproteminaemy occurs - an event, singled out the by Soviet author L.M. Model as the root of the disease of tuberculosis. It is impossible in this short presentation to go into greater detail. Let's, however, bear in mind that the amino acids, which are the most important in the medical nutrition - tryptophan, tyrosinc, phenylalaninc - are separated during the digestion of edestin first. Furthermore, the arginin, cystein and alaninc content in edestin is much higher than in other proteins of plant or animal origin. Finally, amino acids, which are in edestin in smaller quantity than in proteins of animal origin, can be easily replaced in medical nutrition by cottage cheese. There are plenty of reasons why hemp seed edestin should be, in addition to cottage cheese, egg yolk and oat gluten, included among the most important components of medical nutrition for patients with tuberculosis.
As we have witnessed in conjunction with the other proteins, it is of great importance, particularly in the case of edestin, to maintain it in colloid state. From this point of view, our product EDEZYM (the name originated from two words: edestin and enzyme), was very suitable. It has been available on the market for a number of years, though was discontinued after the nationalization of the pharmaceutical industry, in 1948. We may use, however, a simple home preparation, assuming that we have a high quality hemp seed, no older than two years, in which all the proteins and enzymes are still fully active (in order to find out we may conduct a germination test). Old recipes, in which our forefathers prepared the hemp seed soup or porridge, are not useful anymore. In the majority of cases, they lead to coagulation and denaturalization of edestin. ln the preparatory stage we have to remove the outside layer of the seed, which in contrast to oats, is indigestible, discourages the intake and is irritating during the digestion. The only remaining solution is to transfer the content of the seed into a colloid solution and remove the indigestible residue by pressing and sifting.
The best method is based on the extraction of ground hemp seeds by hot milk (60-80 degrees C). The content is constantly mixed while it is kept in a water bath (double boiler), which prevents the excessive heating of the bottom of the container. If this is not done properly, edestin starts to coagulate from the bottom. Sometimes it fully coagulates. Milk could be skimmed, but must be fully fresh and without preservatives. Sweet whey may be used as well. We can obtain it by the coagulation of casein with chymosine. Maceration of the hemp seed, at the above mentioned temperature. should last at least half an hour, preferably more. The finished colloid must be aggressively pressed, filtrated, in some cases mildly sweetened and offered to the patient either immediately or kept at a temperature of 60 degrees C in a water bath, until used. This will prevent hydrolics or fermentative breakdown of the active components. One dose, prepared from 3/8 litre of milk and 50-80 grams of hemp seed, should be consumed by the patient every second day on an empty stomach.
V.
The human organism is capable of dealing, under favourable conditions and to a certain level, with the tuberculosis illness without particular treatment. During times, when calmetisation was unknown and modern antibiotics and tuberculostatics were not available, the majority of primary effect cases were healed spontaneously, at least as far as children beyond the baby stage are concerned. Certainly, the modern organization of the fight against tuberculosis (calmetization, the introduction of child preventative medicine, regular Rig check-ups) lead to a significant reduction in small children morality and proving that we can't rely too much, or exclusively, on the spontaneous healing and protective properties of the child's organism.
This is more true in cases of post primary (secondary) child tuberculosis of lungs and Iymphatic glands. Here, as well, we can see a significant tendency for spontaneous healing, but the assumption of favorable conditions plays a decisive role. lt was for this reason, that during the not so distant past, the cases of "secondary" lung tuberculosis, prevalent in children of school age,the mortality level was rather high, namely among poor people.
This fact underlies again the importance of living conditions. In mature individuals (therial lung pthisis), though the spontaneous healing of lung damage is much rarer than in children, it is much more probable where the living conditions are more favourable. lt is for this reason, that a higher percentage of mature people were saved from the upper layers of the society.
lt is true, however, that wealth and poverty must not necessarily synonymous with good and bad living conditions. But, in contrast to the present days when living conditions in our countrv are more or less uniformly provided, wealthy people were able to assure for themselves favourable living conditions, assuming they understood what represents "true favourable living conditions". Money without knowledge is not enough. The knowledge, which is required, is defined in every time period by the scientific content of the term "hygienic-dietetic healing".
The substance of this "term" developed historically, is changing constantly and will, in conjunction with the general scientific development, continue to change always. It was not a long time ago, when overfeeding a patient suffering from tuberculosis, without taking into consideration the effect on the liver function, was considered purposeful and desirable. Today we have corrected many things, however, many more cry for change. The fast and successful development of "active" treatment methods seems to absorb excessively the attention of ftisoclogs and this leads to insufficient interest in systematic improvements and scientific involvement in hygienic-dietetic methods. This is happening at times when nobody denies that even the most effective "active methods" must be supported by hygienic-dietetic methods, the necessary foundation of all anti-tuberculosis treatments.
Why, then, despite all the progress in "active" therapy, do the hygienic-dietetic methods (foremost the medical nutrition) remain the necessary foundation of all treatments? Why from those methods (and specifically from them) do we expect the fulfillment of the favourable conditions, which make the treatment much easier, and which in some cases, make spontaneous healing possible?
To generate or restore such conditions, during which the human organism is capable of dealing successfully with the disease, is the main mission of hygienic-dietetic treatment and specifically the medical nutrition. lf we are successful and wish to call the resulting healing process "spontaneous" it is only a question of suitable terminology.
If; by using the certain system of medical nutrition, we achieve, in the treatment of tuberculosis, spontaneous healing with considerable probability or regularity, and if we, at the same time. achieve a restitution of the overall nutritional state, during which the tuberculosis slowed down and decreased, then we have solved our problem. This means that we have found the favourable conditions, under which the human organism can better resist the tuberculosis, or deal with it successfully.
VI.
As a testing stone of such systems of medical nutrition, we can best use the cases of post primary (secondary) child tuberculosis of lymphatic glands and lungs, accompanied by substantial degradation of total nutritional status of body development. Such cases tend to show a substantial tendency towards "spontaneous healing', assuming that the living conditions are favorable. If we can achieve, in such cases, dramatically favourable turns for the better as far as the healing of the lung damage and as far as the nutritional status and body development is concerned, then we have, with the highest probability, presented a proof that the system we have used represents the "favorable conditions".
In the following part, I present two groups of children which will offer the necessary documentation for this case.
The first group of 16 children (8 boys and 8 girls) was treated in Jince sanitarium in 1938. In this difficult period, when the sanitarium - at that time a private enterprise - was, because of the world's economic crises, basically idling. Faced with the threat of Hitler's occupation, I have offered the Red Cross in Prague an expense free stay and treatment for 20 children with tuberculosis. In a few days we filled the first floor of the building by these, exceptionally welcomed guests, sick members of Prague's poor from the following districts: Nusle, Pankrac, Michle, Kosire and Kobylisy. After a few days we excluded four of the 20 children and returned them back to Prague. Two were excluded because we did not diagnose any active tuberculosis changes and two others for other reasons. The remaining 16 children remained under treatment for various lengths of time, as is discussed later.
The children came to us in a state of more or less depressed nutrition. The tuberculosis (primary and secondary) was confirmed and checked by the Prague doctors, from whom we received the children.
While with us, the children (as well as the mature patients) were offered meals three times a day. They drank only during the meal. There could be no doubt that they were not overfed. Once a day, they had the main meal, based on meat. once a day they received 100 g of cottage cheese, 25 g of cream (in Czech: "rozhuda"). Once a day they were offered oat porridge made from 15 g of oat flakes. At noon, always after they consumed soup, they received 75 g of shredded carrots with few drops of lemon juice and a soup spoon of cream. Twice a day they received 100 grams of fruit, twice a day 20 g of fresh butter from a farm. Otherwise they received mixed home meals with one limitation. All foods, which would have excessively burdened the liver, were excluded.
The children did not use any other medication, with the exception of colloidal extract of hemp seed. EDEZYM, which was described in part IV. Three times a day the children received soup spoon of Edezym, always a quarter hour before the meal (without a drink), then vitamin B1 and vitamin C. They received two tablets daily, though the food was rather vitamin rich.
The lack of appetite and fussiness toward food, characteristic in children suffering with tuberculosis, was gone in all children, without exception, during the first days of treatment. We also noticed in all children from the first days, a distinct and pervasive change in the total health status.
The boys gained on average 1 kg. within 14 days; girls within 20 days. Boys increased their height by 1 cm in 35 days, girls in 38 days. The diameter of the rib cage was increasing in boys by 1 cm in 18 days, while in girls in 20 days. This improvement in the total physical state and body development in all 16 children is obvious from the pictures, made at the beginning of the treatment. Together with the data, collected from individual children, they are presented in the following overview:
Since the whole group of 16 children were treated at the same time and by the same method, with results indisputably positive there is no doubt. that the treatment was effective. The food, offered three times a day, was neither more abundant or calorically richer than the one which was offered in other institutions and in a majority of families where a child was identified as sick and in need of substantial nutrition. On the contrary, at those institutions we could talk about overfeeding, where meals are presented five or six times a day and the caloric value is higher.
The calories on the plate are not helping if we can't formulate the diet in such a way that the nutrients are utilized and assimilated. Our approach can be summarized in three parts:
1. Preventing overburdening of the liver and other digestive and metabolic organs with harmful foods, offered too frequently. We are trying to encourage their proper functioning by offering some ingredient with specific properties (vitamins and others).
2. We are offering, if possible at every meal, some of the "plastic" proteins, which we have recognized as being natural building material, essential for the formation of animal and plant organisms (cottage cheese, egg yolk, reserve proteins from various plant products, cereal and specifically oat gluten, edestin from hemp seed).
3. Such "plastic" proteins are offered in seemingly small daily doses (for instance 100 g of cottage cheese, I yolk, a few nuts, barely 15 to 20 grams of oats and same amount of hemp seed) but in colloid form, not denaturalized and not coagulated.
The importance of such modified and with hemp seed edestin supplemented medical nutrition will be even more obvious, when we realize, that it was the only substantive base of the whole treatment. During this medical nutrition, we have supplemented the diet with EDEZYM, and not used other medication or medical treatment. ln 1932, other effective medications against tuberculosis were not even available.
The other 10 cases represent a looser group of children and teenagers who were treated during the second world war - during the occupation. Only one case took place earlier, in 1933, and this girl (11 year old Maria Plecita) was included to this group as, with exception of the time the treatment took place, all the other factors (pathology, therapy) were the same as for the remaining 9 children in the group.
During this period the sanitarium was fully occupied by mature patients, only five years old Ludek Ledecky undertook the treatment together with his father, suffering with tuberculosis as well. Others were treated at home, under our ambulant supervision. Even this group does not represent specific selection, it included all children we have ambulantly treated. They were considered altogether exceptional.
The level of the nation's nutrition during this period was not good and the children under the home regimen were missing many things, which the sanitarium had in abundance for the children in the first group, in 1938. There was no cream. The cottage cheese was also in short supply and when the parents of the small patients were able to acquire it, the quality was low, as it was hard and coagulated. There was a shortage of butter and high quality fats in general. Similarly, quality meat and sometimes even eggs, sugar and other important food ingredients were not available. Such nutrition was inadequate even for healthy people but even more so for the sick ones. This hard time, however, left our patient two things, which, in addition to cottage cheese, were perhaps the most important: oat flakes and EDEZYM. Consequently, we have been able, during this difficult period and with half way correct home diet, to achieve with this second group of children convincing nutritional and treatment results, equal to the ones achieved in 1938.
These cases. which were part of the second group, took place when the children were not even protected by "calmetisation" or could have been saved by chemotherapy, or by antibiotics. It is obvious as well, that at that time, we didn't have at our disposal detailed diagnostic analysis of individual cases, which would satisfy today's requirements of phthisiology. In particular, we did not have the tomographic data and so we have only estimated, using X-ray pictures, where the atelectasc ends and the inflammation changes begin, when and to what extent we can demonstrate break up and where the dissemination took place. Nevertheless, even this norrnal skiagram brings sufficiently convincing evidence, that to all children in this group, the treatment brought about a significant turn over in the disease, which was, up to this point, considered "progressive". This means that it brought about a regression of the pathological changes in glands and lungs and, in the majority, also a distinct "restitution and integrum". If we add to it that paralicly with the positive development of the lung finding. We have seen in all children, right from the beginning, a similarly positive change in the total health status, which had, before the treatment started, deteriorated progressively. It was clear that to bring about full curative and nutritional effects, even the little which remained available from our medical nutrition during this war period (oat meal, hemp seed, a little cheese, a few yolks, and protection of the liver) was sufficient and that in this "little" is the substance of the effective factor.
In the following table, we have summarized the curative effects. which were achieved by the treatment of the second group of ten ambulantly treated children. The summary deals with the effects of lung findings and the total nutritional state and development:
On a group of twenty-six tuberculosis stricken children and teenagers, presented in two groups in "as the herd is running" fashion (this means without any selection), we have been able to achieve positive results. From the point of treatment, nutrition, or physical development, medical nutrition, supplemented with the hemp seed edestin, had an unambiguously favorable effect.
The attached documentation, generated ten to twenty years of age, will not meet today's requirements of the phthisiology. It leaves in some cases doubts if the described type of pathological change or group of changes was or was not of the specific type. There is, however. not a slightest doubt about the following:
1. All children were included into our treatment program in the state of progressive worsening of total health status and also in the majority of cases with documented lung disease;
2. In all participants this treatment immediately caused a turn over in the sense of regression of changes caused by the disease and improvement of the overall health status;
3. In all cases, without any other medication or treatment procedures, within a usually short time, a healing of the lung or glands disease was accomplished. And, during the same short period of time, with only three meals a day, not excessively rich, a farreaching restitution of the nutritional status and physical development was noticed.
Out of these facts it is obvious that this treatment of medical nutrition proved to be good and very effective. It was happening in a time period when similarly effective means of treatment were not available. In this sense, the treatment was saving the lives of children threatened by tuberculosis (as well as mature people) and was in a position to save many more if it only received the deserved attention.
In the first group of 16 children belonging to the poor people of the Prague suburb, somebody may have commented,that the turn over in their health status was influenced by removing these children from unhealthy living conditions and housing them in a hygienic and rather "affluent environment". It could not be denied that this was an important factor, which had a positive influence, it has an effect during each transfer of a sick child into a hospital, however, we don't see in every case such a change. We do not see such a straight forward means. As well, this objection loses it merit when we compare the first group of children with the second group which, with only one exception, did not changed their environment, but were treated at home.
Moreover, this relatively "affluent environment" was often restricted by the miserable economic condition during the war. Despite that, in such unfavorable conditions, we witness the same convincing and unambiguous results, the same overall improvement.
It is exactly this comparison of the two groups of children which leads us to the discovery of the factors which were effective in the treatment of both groups. For certainly, it was not the effect of the changed environment and "comparative affluence" which we provided for the children in the first group, but which was not available for the children in the second group. It must have been the parts of the treatment which were available to both groups. From the effective substances we should name: porridge from the oat flakes, EDEZYM from the hemp seeds, and cottage cheese. Further, we should add the protection of the liver, which means the exclusion of meals which are overburdening the liver and the exclusion of frequent presentations of meals and drinks.
If we take the preservation of liver as a logical part of the patient's hygiene, we can condense the whole topic to three factors: oatmeal porridge, EDEZYM and cottage cheese. It is not to say that raw or "soft" egg yolk, nuts, raw vegetables and fruits and other, previously discussed things are not important. But the most important, as we can conclude from our analysis, are the three: oats, hemp seed and cottage cheese. And, we repeat, that all three must be prepared in such a way that the proteins will be colloid, under-naturalized and in a non-coagulated state. All other effective substances of the medical nutrition could be, more or less, missed by the patient, as they were missed by the children in the second group, without endangering the results of the medical nutrition. If, however, one of the three basic pillars of the treatment is missing, or is damaged (denaturalized) by the improper processing, the results of the treatment are half as effective or less effective.
Today, when we don't have EDEZYM and the cottage cheese is sometimes of poor quality, we have Streptomycin, PAS, and INH, in addition to surgical methods. Let's be careful, however! A conscientious doctor always considers the strong points and weaknesses of such medications and while treating the mature patients, or even more, while treating the children, he uses them only in cases where they are needed and in doses which are tolerable. If he understands the importance of liver protection, he is twice as careful, particularly when dealing with para-aminosalicylic acid. And makes sure "that he will not use all his ammunition before the main battle starts". This means he avoids the frivolous use of full doses of antibiotics and bacteriostatical drugs, so that in case of exacerbation or recidivity, he will not be without an effective weapon. All such unavoidable considerations must reinforce our conviction, that a means which is relatively effective and at the same time absolutely harmless when used for an extended and unlimited period, as is our medical nutrition, should not be overlooked even today, in a time of antibiotics.
We, in Jince, even today subject our patients, who are mature and chronic, to the appropriate preparation before we will use antibiotics or tuberculostatics. Those who need it, will be educated in the proper order in eating and drinking. Smokers are retrained into non-smokers and all are included into a regimen of liver protection. Usually, we achieve, particularly in disciplined patients, a nice improvement, without medication. Only in cases when the treatment progress is slow, do we, after careful consideration, use antibiotics and bacteriostatics. Patients will, however, always be supported by medical nutrition. This medical nutrition is an essential part of our patient's education while they are being treated at home.
SUMMARY
The use of hemp seed in the therapy of tuberculosis is based on our experience of the last thirty years, gained at Jince in the area of medical nutrition. In the proper function of the liver we have always seen a precondition for perfect assimilation of nutrients. For this reason we have emphasized the rules and limitations which we know today as the foundation of liver diet. We consider them to a certain point as a universal base of every medical diet. Medical nutrition during tuberculosis must stress, in addition to vitamins B1, C and A, primarily proteins and among them namely those which nature destined to serve as building material for the formation of organisms. Such protein sources, for instance, include cottage cheese, egg yolk, reserve proteins in cereals, nuts and other fruits. It is of great importance. that such proteins are processed without denaturalization. Professionally prepared cottage cheese is a precious dietetic component, but hard and coagulated is dietetically worthless. Similarly, raw egg yolk is a good, but boiled to hard state is not. A daily does of only 10 to 20 grams of oats, in the form of professionally prepared porridge will soon prove its medicinal properties, while twenty times higher doses of cereals denaturalized by baking or cooking in water have a dietetically rather indifferent affect. The ground hemp seed, extracted with milk, heated to a temperature between 60 to 80 degrees C will have, even in such small doses, an important healing effect. We are convinced that a child with tuberculosis is the best testing ground for medical nutrition based on hemp seed.
Source: hemphearts.com/HempHeartsStudy.pdf