Imhigh85
Well-Known Member
Sweetsue I am stopping by in your Journal to see how everything is going maybe learn a few new things along the way but I'm here to say that I will be subscribing and you will see me from time to time
How To Use Progressive Web App aka PWA On 420 Magazine Forum
Note: This feature may not be available in some browsers.
Sweetsue I am stopping by in your Journal to see how everything is going maybe learn a few new things along the way but I'm here to say that I will be subscribing and you will see me from time to time
 My regular journal is my grow journal, the link to which you'll find in my signature. I'm happy to have you stop and engage in any of the threads.
My regular journal is my grow journal, the link to which you'll find in my signature. I'm happy to have you stop and engage in any of the threads. 

Yeah I'm not very good with technology I suck eventually I will wander around and find your thread like I found this one but I appreciate it I tried
Here, this is a link to the current page of the grow journal. No one expects you to read through or try to keep up with the manic pace, but we sure have fun together, and you're more than welcome to join in. 
 There's a two to three-day build up with enticing promises in a slick video presentation that left me in awe of the woman's ability to transmit authenticity. I have no doubt she's an effective mentor, but I feel about this the way I feel about Christianity, or for that matter any religious message.
There's a two to three-day build up with enticing promises in a slick video presentation that left me in awe of the woman's ability to transmit authenticity. I have no doubt she's an effective mentor, but I feel about this the way I feel about Christianity, or for that matter any religious message. 


Anandamide and anxiety with particular attention to PTSD - Nancy Minyanou in fulfillment for a class requirement.
"This video plans to give evidence that modulation of anandamide Cann be a powerful treatment for anxiety disorders, such as PTSD, for its effects on anxiety behavior and memory consolidation.
Amandine is an endogenous endocannabinoid, also known as AEA. It is an L-peptide linking polymer of amino acids, according to the Protein Data Base's ligand entry.
Cannabinoid agonists have a bi-physic reaction such that higher doses are associated with having an anxiety-inducing effect, where lower doses have an anti-anxiety effect.
Receptor type 1 activation reduces GABA release from pre-synaptic terminals, increasing cell excitability.
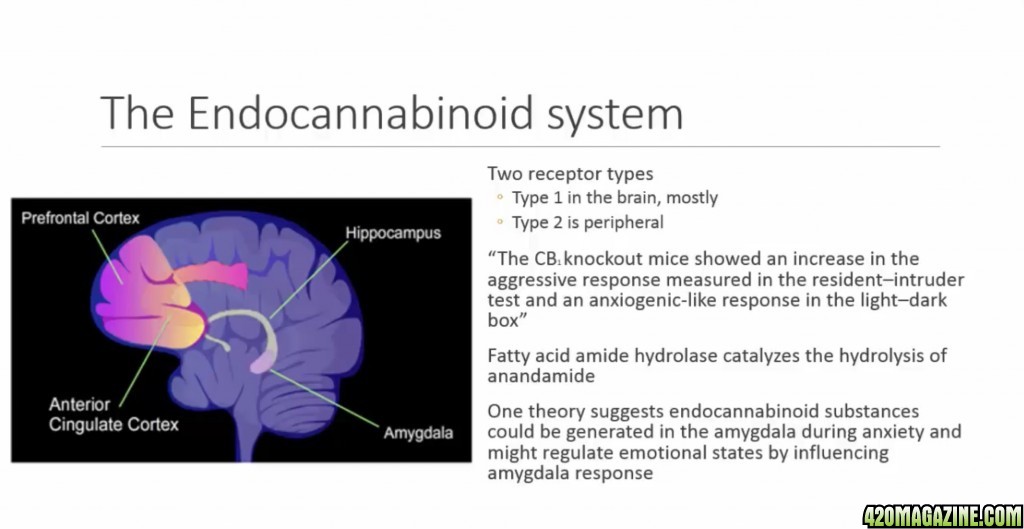
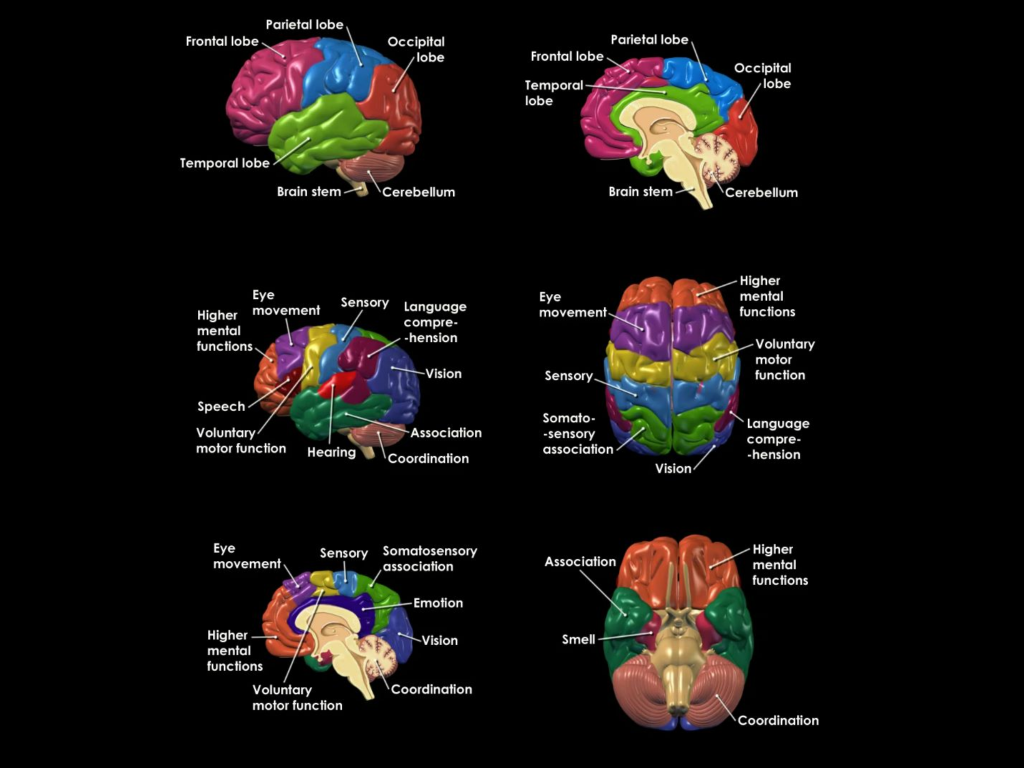
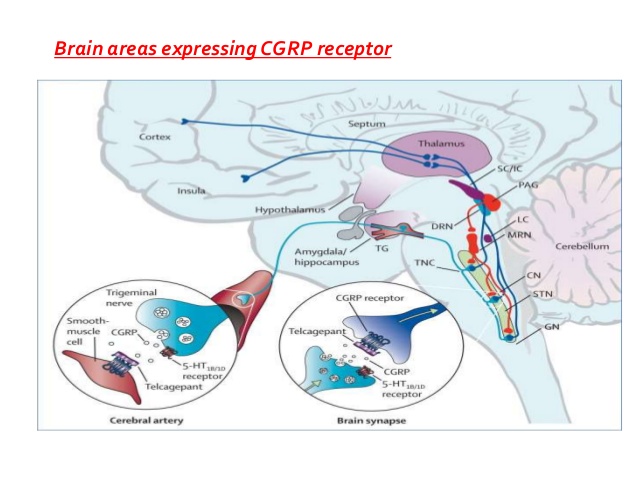
Type 1 is most densely found in the amygdala, hippocampus, anterior cingulate cortex, and prefrontal cortex, all important regions for anxiety regulation.
Type 2 is found periferally.
Experiments suggest that endogenous cannabinoids have a hand in regulating emotional behavior. There appears to be a functional relationship between cannabinoid CB1 and 5HT1A receptors in modulation of adrenal cortical activity.
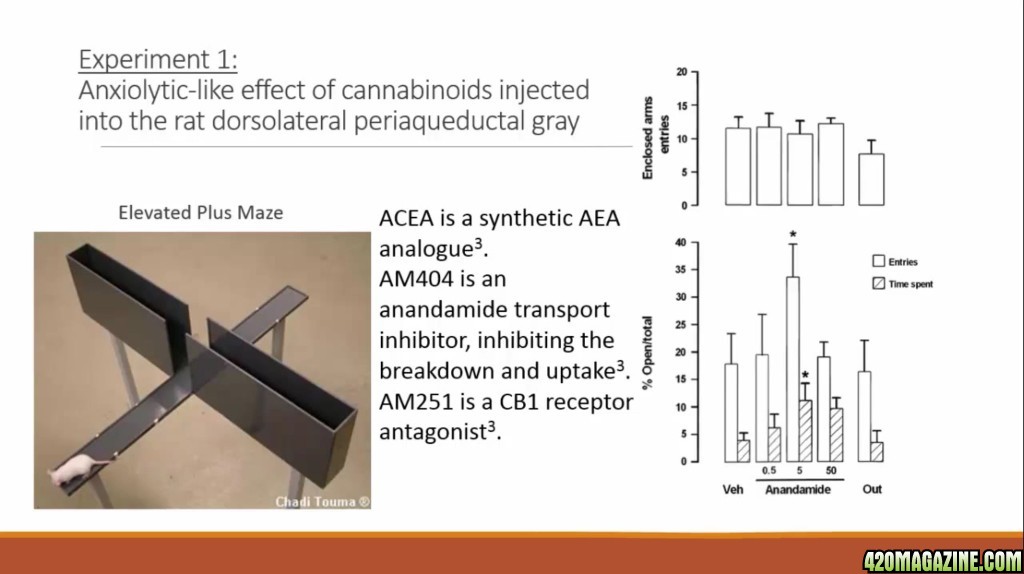
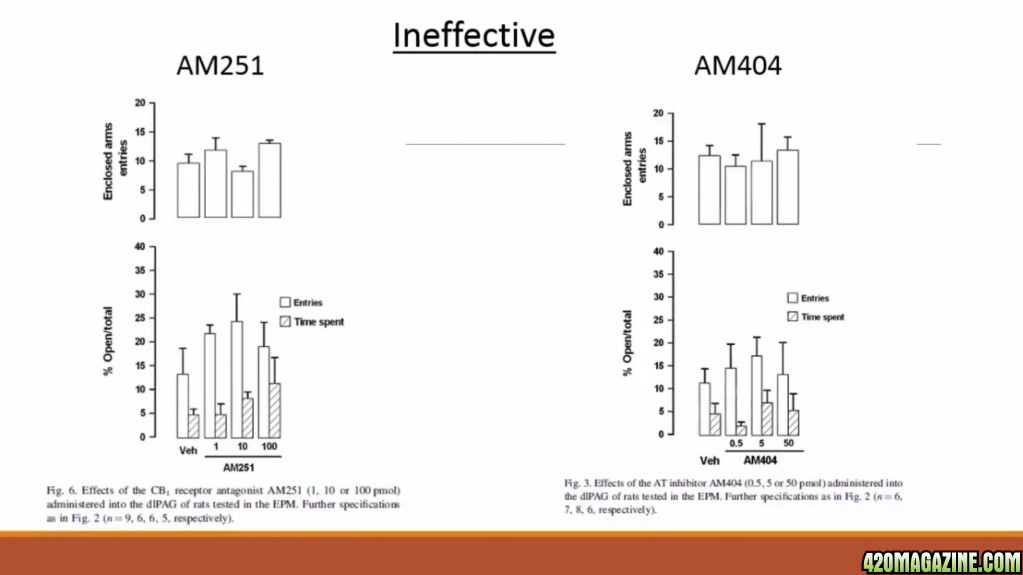
AM 404, an anandamide transport inhibitor, inhibits the breakdown and uptake of AEA. AM251 is a CB1 receptor antagonist.
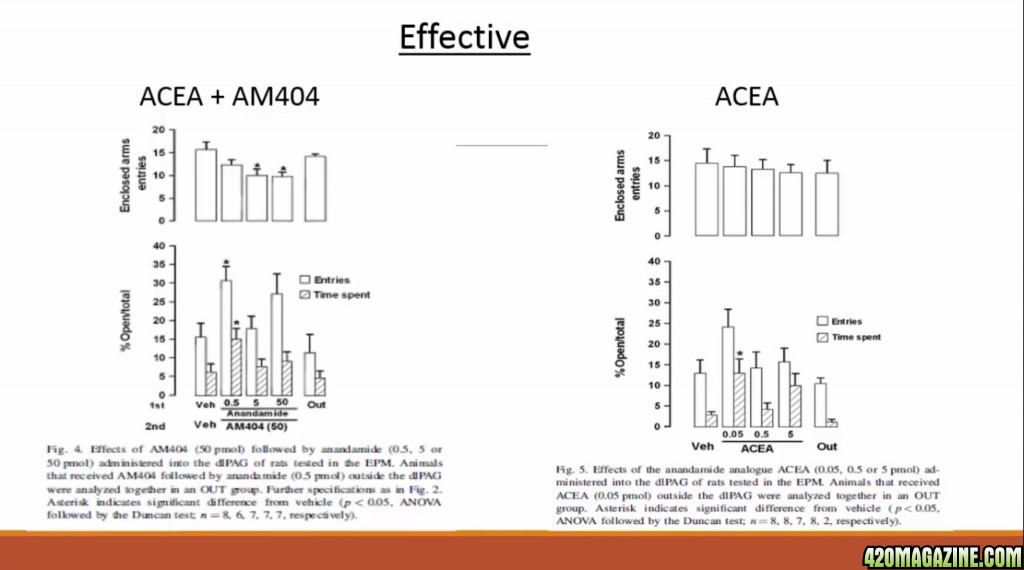
AEA-injected rats spent more time on the elevated arms with lower doses, and after they were first injected with AM404.
Using ACEA alone or with AM404 resulted in a bell-shaped response curve.
Neither AM251 or AM404 were effective alone in modifying animal behavior.
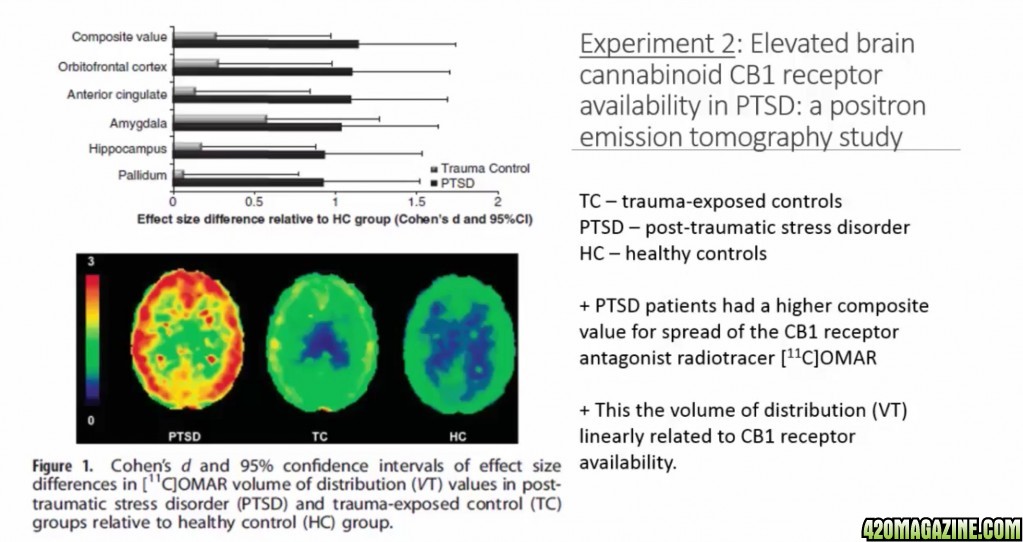
Peripheral levels of AEA and other compounds were assessed in healthy individuals, those who had experienced trauma, and those with PTSD, which is more pronounced in women.
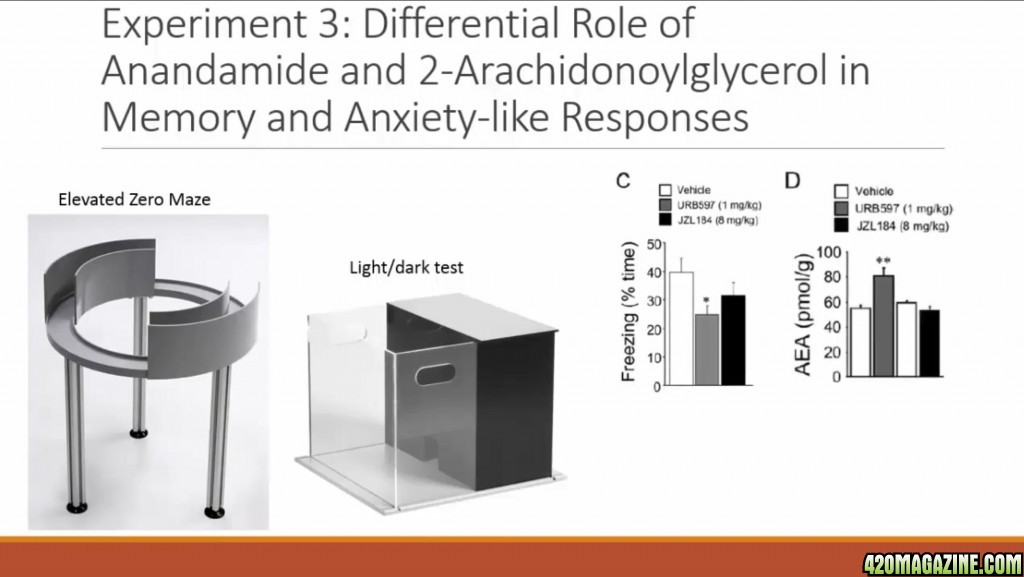
the elevated +/0 mazes were used to test for anxiety via time spent on open sections of the platform. The acetic acid test performed had mice injected with acetic acid and the number of reads was counted to measure nose inception(??????)
Fear, conditioned to object and context recognition was used to test the effects of URB597 on memory consolidation. Graph C's middle bar shows a lowered freezing after given URB597. Graph D shows the increased level of AEA after administration of URB597. It inhibits the AEA degradation enzyme, fatty acid amide hydrolase. It produced anxiolytics effects in both mazes through the activation of different cannabinoid receptors, suggesting CB2 being a good target for future treatment of anxiety disorders and modified brain content of AEA.
They found that URB597 mediated modulation of ARA promotes memory deficits through similar mechanisms as that for THC, the psychoactive component of cannabis.
), and Protection. Rest, Eat, Sleep, Forget, Protect
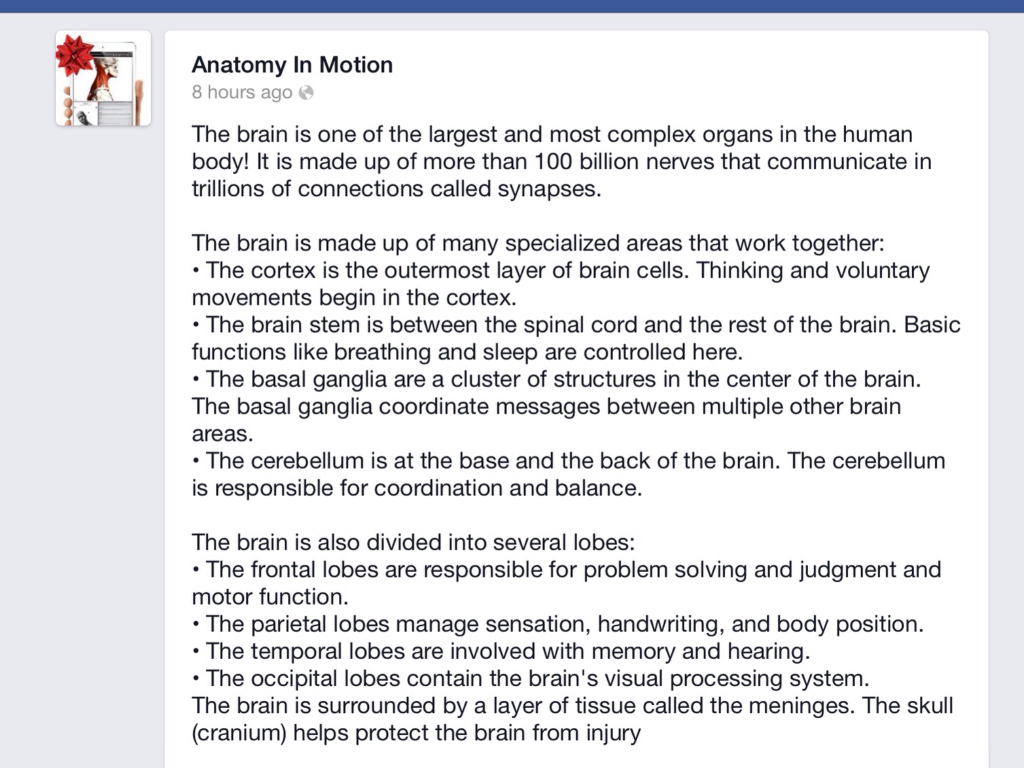
 They suppress the respiratory center of the brain and your body forgets to breath. Dammit!! Stopping at 6:56. I'll pick up tomorrow. I'm seeing double. Lol!
They suppress the respiratory center of the brain and your body forgets to breath. Dammit!! Stopping at 6:56. I'll pick up tomorrow. I'm seeing double. Lol!  ), and Protection. Rest, Eat, Sleep, Forget, Protect They depress the respiratory center of the brain and your body forgets to breathe.
), and Protection. Rest, Eat, Sleep, Forget, Protect They depress the respiratory center of the brain and your body forgets to breathe.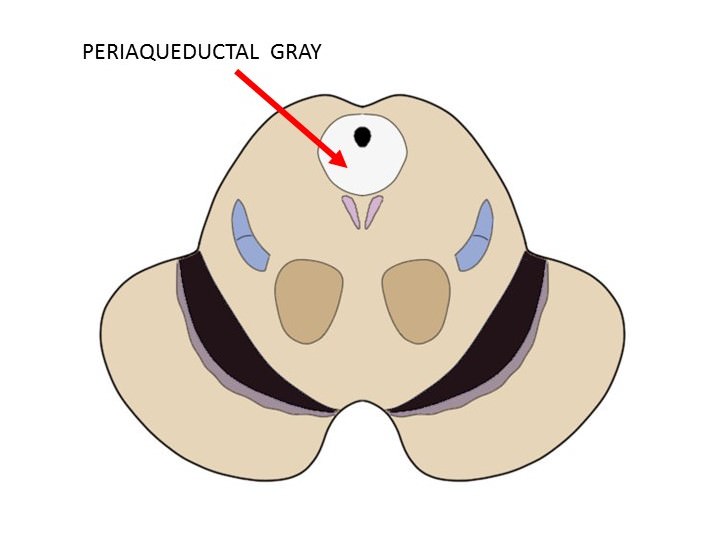 ), and Protection. Rest, Eat, Sleep, Forget, Protect They depress the respiratory center of the brain and your body forgets to breathe.
).
), and Protection. Rest, Eat, Sleep, Forget, Protect They depress the respiratory center of the brain and your body forgets to breathe.
).
 Start again woman!
Start again woman!