- Thread starter
- #61
Compliments of Tiffany, the Wake + Bake intern:
WHAT IS CBD?
I imagine CBD to be THC’s rad side kick and they are working together to make us feel better. That’s not to downplay the many other superhero cannabinoids in cannabis… but, CBD and THC are the primary ones.
Common ways of ingesting CBD are with tinctures, CBD oil, capsules, vaporizing or smoking, CBD topicals (lip balm, lotions, etc.), and even suppositories.
The Benefits of CBD
We’ve only begun to uncover the medicinal benefits of CBD. Here are some of the proven effects of CBD.
Anti-inflammatory
Combats inflammatory diseases such as, Irritable bowel syndrome (IBS), arthritis, fibromyalgia
Anti-tumoral/anti-cancer
Proven to shrink breast cancer cells and prevent them from growing
Combats tumor and cancer cells
Anti-psychotic
Combats psychotic disorders; such as, schizophrenia, delusional disorder, psychotic disorder
Anti-depressant
Combats mood disorders; such as, bipolar/manic depression, PTSD, panic disorder, addiction
Analgesic
Reduces chronic pain or pain that can be caused by many kinds of illnesses; such as, diabetes, fibromyalgia, IBS, etc.
Antiemetic
Reduces nausea caused by cancer, mood disorders, IBS, other digestion issues, etc.
Anxiolytic
Combats anxiety disorders; such as, Post Traumatic Stress Disorder (PTSD), panic disorder, Obsessive Compulsive Disorder (OCD), etc.
Antioxidant
“Protects body from damage caused by harmful molecules that can cause cancer.” – WebMD
Combats neurodegenerative disorders such as; Parkinson’s, Alzheimer’s, Huntington’s
Protects memory
Helps with Diabetes
Improves insulin levels, reduces blood glucose levels, reduces blood pressure and reduces inflammation
Anticonvulsant
Suppresses seizure activity caused by: seizure disorder, epilepsy
In 2007, there was a study at the California Pacific Medical Center in San Francisco done by Dr. Sean McAllister and some of his colleagues. They reported on how effective CBD can be when being used to kill breast cancer cells. According to ProjectCBD, “CBD destroys breast cancer cells by down-regulating a gene called ID-1, which is implicated in several types of aggressive cancer. Silencing the ID-1 gene is, thus, is a potential strategy for cancer treatment.”
CBD is Commonly Used for the Following Conditions
* Cancer
* IBS
* Diabetes/Metabolic Syndrome
* Fibromyalgia
* Chronic Pain
* Nausea
* Arthritis
* Anxiety/Mood Disorders
* Epileptic Disorders
* Parkinson’s Disease
* Chronic/Neuropathic pain
* Overcoming addiction (to things like: cigarettes/nicotine, opioids, alcohol, etc.)
WHAT IS CBD?
I imagine CBD to be THC’s rad side kick and they are working together to make us feel better. That’s not to downplay the many other superhero cannabinoids in cannabis… but, CBD and THC are the primary ones.
Common ways of ingesting CBD are with tinctures, CBD oil, capsules, vaporizing or smoking, CBD topicals (lip balm, lotions, etc.), and even suppositories.
The Benefits of CBD
We’ve only begun to uncover the medicinal benefits of CBD. Here are some of the proven effects of CBD.
Anti-inflammatory
Combats inflammatory diseases such as, Irritable bowel syndrome (IBS), arthritis, fibromyalgia
Anti-tumoral/anti-cancer
Proven to shrink breast cancer cells and prevent them from growing
Combats tumor and cancer cells
Anti-psychotic
Combats psychotic disorders; such as, schizophrenia, delusional disorder, psychotic disorder
Anti-depressant
Combats mood disorders; such as, bipolar/manic depression, PTSD, panic disorder, addiction
Analgesic
Reduces chronic pain or pain that can be caused by many kinds of illnesses; such as, diabetes, fibromyalgia, IBS, etc.
Antiemetic
Reduces nausea caused by cancer, mood disorders, IBS, other digestion issues, etc.
Anxiolytic
Combats anxiety disorders; such as, Post Traumatic Stress Disorder (PTSD), panic disorder, Obsessive Compulsive Disorder (OCD), etc.
Antioxidant
“Protects body from damage caused by harmful molecules that can cause cancer.” – WebMD
Combats neurodegenerative disorders such as; Parkinson’s, Alzheimer’s, Huntington’s
Protects memory
Helps with Diabetes
Improves insulin levels, reduces blood glucose levels, reduces blood pressure and reduces inflammation
Anticonvulsant
Suppresses seizure activity caused by: seizure disorder, epilepsy
In 2007, there was a study at the California Pacific Medical Center in San Francisco done by Dr. Sean McAllister and some of his colleagues. They reported on how effective CBD can be when being used to kill breast cancer cells. According to ProjectCBD, “CBD destroys breast cancer cells by down-regulating a gene called ID-1, which is implicated in several types of aggressive cancer. Silencing the ID-1 gene is, thus, is a potential strategy for cancer treatment.”
CBD is Commonly Used for the Following Conditions
* Cancer
* IBS
* Diabetes/Metabolic Syndrome
* Fibromyalgia
* Chronic Pain
* Nausea
* Arthritis
* Anxiety/Mood Disorders
* Epileptic Disorders
* Parkinson’s Disease
* Chronic/Neuropathic pain
* Overcoming addiction (to things like: cigarettes/nicotine, opioids, alcohol, etc.)
 I couldn't be happier to help you gain more understanding of how marvelously your body works and how powerful the healing force within you is.
I couldn't be happier to help you gain more understanding of how marvelously your body works and how powerful the healing force within you is. 



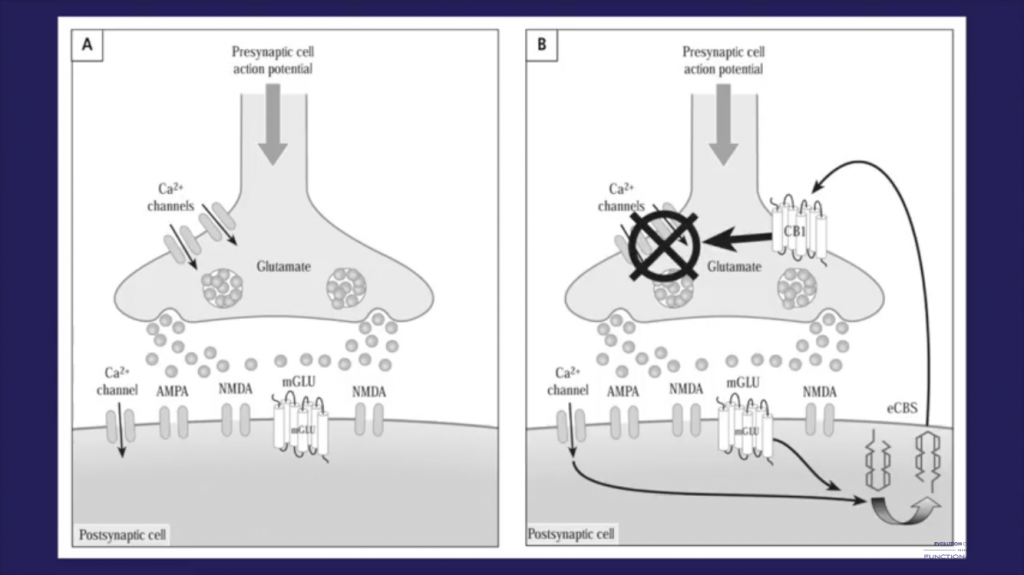
 "So having this auto-protective, negative feedback mechanism...so this is very different to how typical neurotransmitters work.
"So having this auto-protective, negative feedback mechanism...so this is very different to how typical neurotransmitters work.